Infants and young children are in a period of visual development, but even if there are developmental problems, they are not aware of them, and unless the visual impairment is severe, family members often do not notice. For example, with infantile strabismus, there is a common belief that “it will get better on its own,” which can delay consultation. To prevent such delays, infant health checkups are very important.
Visual function reaches nearly adult levels by around age 3–4. Amblyopia detected during this period (especially refractive amblyopia or anisometropic amblyopia, which are not visible externally) responds well to treatment and has a high chance of reaching normal vision by school age.
The prevalence of amblyopia is reported to be about 1–5% 1). Since early detection and treatment greatly affect visual prognosis, it is important for parents, caregivers, and school personnel to understand the signs of vision problems.
The proportion of individuals with uncorrected visual acuity less than 1.0 is increasing. In junior high and high schools, the rate of “uncorrected visual acuity less than 1.0” is the highest (School Health Statistics, FY2014).
School Type
Uncorrected Visual Acuity < 1.0
Uncorrected Visual Acuity < 0.3
Kindergarten
26.53%
0.97%
Elementary school
30.16%
8.14%
Junior high school
53.04%
24.97%
High school
62.89%
35.84%
The vision screening implementation rate in kindergartens is only 48.3%, below 50% (Japan Ophthalmologists Association, 2008 survey), indicating that vision abnormalities are not sufficiently detected at the kindergarten stage.
QHow common is vision loss in children?
A
About 30% of elementary school students and about 53% of junior high school students have uncorrected visual acuity below 1.0 (School Health Statistics). Amblyopia is found in about 1-5% of children 1), and as poor vision that cannot be improved with correction, early detection is particularly important. Increasing the participation rate in three-year-old health checkups and school health checkups leads to early detection of vision problems.
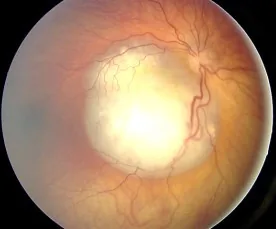
Dimaras H, et al. Retinoblastoma. Orphanet J Rare Dis. 2006;1:31. Figure 2. PMCID: PMC1586012. License: CC BY.
Fundus photograph of retinoblastoma showing whitish tumor tissue on the retina. Corresponds to the white pupil (pupil appearing white) discussed in section “2. Signs of Awareness by Age and Situation”.
Infancy (0–3 years)
Does not make eye contact or follow objects: If a baby does not start gazing at faces or tracking objects by 2–3 months of age, caution is needed.
Squints one eye or tilts the head: May indicate reduced vision in one eye or strabismus (abnormal head posture).
Seems bothered by light (photophobia): Occurs with glaucoma, corneal disease, or high refractive error.
Watches TV extremely close: May indicate nearsightedness or farsightedness.
Brings picture books or screens close to the face: A sign of reduced vision due to refractive error.
Covers one eye while looking: May indicate anisometropia (difference in vision between eyes) or strabismus.
Tilts the head to see (abnormal head posture): Possible strabismus, heterophoria, or nystagmus. Detailed examination at the 3-year-old health checkup is important.
School Age (6 years and older)
Says they cannot see the blackboard: Corresponds to a vision rating of C to D (0.6 to 0.3 or less) on school vision screenings.
Bringing face close to notebooks or textbooks: A sign of progressing myopia.
Misjudging balls in sports or falling behind in class: Possible binocular vision problems or reduced visual acuity.
Complaining of headaches or eye strain: Often occurs with uncorrected refractive errors (especially hyperopia and astigmatism).
QHow can I notice a child's vision loss?
A
Observe daily behavioral signs such as moving close to the TV, squinting one eye, or tilting the head. Also pay attention to the results (A to D ratings) of the three-year-old health checkup and school vision screenings. If the rating is B to D, see an ophthalmologist early. In particular, whitening of the pupil, sudden vision loss, or eye misalignment may be urgent, so same-day consultation is recommended. Anisometropic amblyopia is not visible from the outside and is easily overlooked even in checkups, so checking vision in each eye separately is important.
3. Basic Knowledge of Amblyopia and Importance of Early Detection
Amblyopia is a condition in which corrected visual acuity is poor despite the absence of organic eye disease. It results from impaired development of the visual cortex due to inadequate visual stimulation during the sensitive period of vision.
If treatment is not started during the sensitive period of visual function (from birth to around 6–8 years of age), amblyopia becomes fixed and recovery becomes difficult. Detection and treatment initiation at age 3–4 offer a high likelihood of achieving normal vision by school age. On the other hand, anisometropic amblyopia is not apparent from appearance and is easily overlooked unless each eye is tested separately during school vision screenings.
Differentiation from Psychogenic Visual Disturbance
Psychological stress can cause temporary visual impairment (psychogenic visual disturbance). Vision loss is often moderate, with complaints such as “I can’t see the blackboard” or “I can’t read the textbook,” but no organic ocular abnormalities are found. Goldmann kinetic perimetry typically shows spiral or tubular visual fields, which is characteristic and important for differentiation from amblyopia.
QBy what age can amblyopia be treated and cured?
A
If treatment is started during the sensitive period of visual function (up to around early elementary school age), there is a high possibility of achieving normal vision. Detection at age 3–4 is ideal, and the prognosis is best when treatment is initiated before school age. After the sensitive period, recovery becomes difficult, so early detection through three-year-old health checkups and school vision screenings, as well as prompt ophthalmological consultation after B or D ratings, is important.
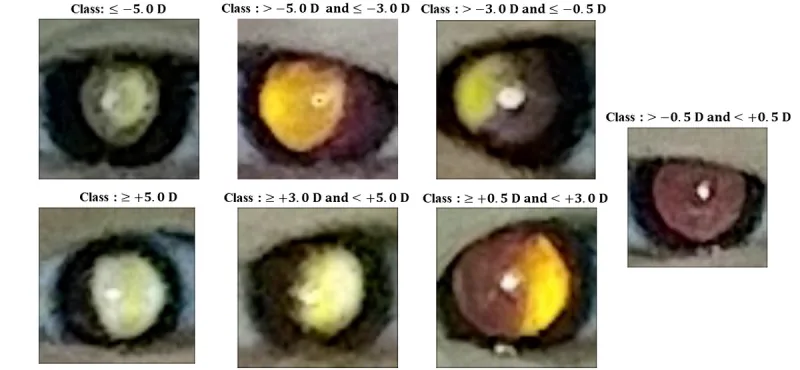
Chun J, Kim Y, Shin KY, et al. Deep Learning-Based Prediction of Refractive Error Using Photorefraction Images Captured by a Smartphone: Model Development and Validation Study. JMIR Med Inform. 2020;8(5):e16225. Figure 3. PMID: 32369035; PMCID: PMC7238094; DOI: 10.2196/16225. License: CC BY.
This image shows the crescent-shaped reflection patterns in the pupil obtained by photoscreening, classified into seven types of refractive errors. It corresponds to the detection of refractive errors using a photoscreener, discussed in section “4. Screening system and examination methods.”
Since 1991, vision and hearing screening has been added to the three-year-old health checkup. At age three, children can communicate verbally and can subjectively report their vision. This checkup is extremely important for detecting visual function abnormalities.
Flow of vision screening at the three-year-old health checkup:
Primary screening (at home): Use of a vision test kit such as a picture vision chart. Parents perform the test at home.
Secondary screening (at the checkup site): Interview and detailed examination (vision, eye alignment, fundus).
In recent years, the introduction of photoscreeners (such as the Spot Vision Screener) has advanced, improving the accuracy of detecting refractive errors and strabismus2). The adoption status varies by municipality, but widespread use in infant health checkups is expected.
Vision Assessment in School Health Checkups (3-7-0 Method)
In school health checkups, vision is tested using the 3-7-0 method (three visual acuity targets: 0.3, 0.7, and 1.0). A visual acuity of 0.7 is considered the minimum level at which a student can roughly see the blackboard from anywhere in the classroom, while 0.3 is the level below which it is difficult to see the blackboard even from the front row.
Judgment
Visual Acuity Range
Meaning / Action
A
1.0 or higher
Normal vision
B
0.9 to 0.7
Ophthalmology consultation recommended
C
0.6 to 0.3
Ophthalmology consultation and follow instructions
D
Less than 0.3
Same as above (urgent consultation needed)
School vision screening also includes eye alignment and eye movement tests. Cover test, cover-uncover test, and convergence test are used to evaluate suspected strabismus or phoria, and consultation is recommended. Color vision testing is not mandatory but can be performed with the consent of the student and guardian.
QWhat should I do if I receive a B to D rating in school vision screening?
A
If you receive a B to D rating, visit an ophthalmologist early. Even a B rating may hide refractive errors (hyperopia, myopia, astigmatism). For C and D ratings, a detailed examination is necessary because of the possibility of amblyopia or organic disease. In particular, anisometropic amblyopia is difficult to detect when viewing with both eyes and is often overlooked in screening, so it is important to have each eye evaluated precisely by an ophthalmologist.
If amblyopia is suspected, cycloplegic refraction with atropine or cyclopentolate is essential. Cycloplegia eliminates the effect of excessive accommodation (pseudomyopia or accommodative hyperopia) in children, allowing measurement of true refractive error.
For children, glasses are the first choice for refractive correction. Contact lens use is increasing (0.2% in elementary school, 6.4% in junior high, 26.6% in high school; 2009 survey), but highly oxygen-permeable rigid lenses or daily disposable soft lenses are recommended for safety.
QCan amblyopia be treated with glasses alone?
A
Refractive amblyopia often improves with glasses alone. In anisometropic and strabismic amblyopia, eye patching (occlusion of the healthy eye) is used in addition to glasses. Depending on severity, occlusion is performed for 2–6 hours per day, and visual acuity improvement is regularly checked. It is important to continue treatment within the sensitive period (until around early elementary school age), and even after visual acuity improves, follow-up may be needed to prevent recurrence.
Visual function develops rapidly after birth, reaching nearly adult levels by age 3–4. This period of rapid development is called the sensitive period (critical period: from birth to around 6–8 years old). If appropriate visual stimulation is not provided during the sensitive period, development of the visual cortex (primary visual cortex V1) is impaired, and poor corrected visual acuity (amblyopia) becomes fixed.
Mechanism of amblyopia onset: Insufficient or uneven visual input → Impaired synapse formation and plasticity in the visual cortex (V1) → Poor corrected visual acuity (amblyopia)
Infants normally have +2 to +3 diopters of hyperopia (physiological hyperopia). With growth, axial elongation reduces hyperopia (emmetropization). If this emmetropization progresses excessively, myopia develops. Increased near work and lack of outdoor activity are known to accelerate myopia progression 4).
During school age, myopia tends to progress easily. Regular eye examinations to monitor refractive changes and, if necessary, updating glasses prescriptions or considering myopia progression control treatments are important.
Myopia is rapidly increasing worldwide, with predictions that about 50% of the global population will be myopic by 2050 5). High myopia (−6D or more) increases the risk of retinal degeneration, glaucoma, and retinal detachment, making progression control from childhood an important issue.
Recommendation for outdoor activity: RCT data show that 2 or more hours of outdoor activity per day suppresses the onset and progression of myopia4). It is thought that high illuminance and high color temperature light in natural light stimulate dopamine secretion and suppress axial elongation.
Low-concentration atropine eye drops: RCT data show that 0.01–0.05% low-concentration atropine eye drops suppress myopia progression by about 50–60%. The LAMP study showed that 0.05% atropine is more effective than 0.025% or 0.01% 6). Side effects such as mydriasis and photophobia are mild at low concentrations.
Orthokeratology: A treatment in which specially designed rigid contact lenses are worn during sleep to reshape the cornea and provide clear daytime vision without glasses. The ROMIO study confirmed a 2-year myopia progression control effect 7). There is a risk of microbial keratitis, so regular eye examinations are essential.
Multifocal soft contact lenses: Evidence for myopia progression control has accumulated, and a 3-year RCT reported a significant inhibitory effect 8).
Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115(7):1229-1236. doi:10.1016/j.ophtha.2007.08.001.
Arnold RW. Amblyopia risk factor prevalence. Journal of pediatric ophthalmology and strabismus. 2013;50(4):213-7. doi:10.3928/01913913-20130326-01. PMID:23556991.
Pediatric Eye Disease Investigator Group.. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Archives of ophthalmology (Chicago, Ill. : 1960). 2002;120(3):268-78. doi:10.1001/archopht.120.3.268. PMID:11879129.
He M, Xiang F, Zeng Y, Mai J, Chen Q, Zhang J, Smith W, Rose K, Morgan IG.. Effect of Time Spent Outdoors at School on the Development of Myopia Among Children in China: A Randomized Clinical Trial. JAMA. 2015;314(11):1142-1148. doi:10.1001/jama.2015.10803. PMID:26372583.
Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j.ophtha.2016.01.006. PMID:26875007.
Yam JC, Jiang Y, Tang SM, et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology. 2019;126(1):113-124. doi:10.1016/j.ophtha.2018.05.029. PMID:30514630.
Cho P, Cheung SW. Retardation of myopia in Orthokeratology (ROMIO) study: a 2-year randomized clinical trial. Investigative ophthalmology & visual science. 2012;53(11):7077-85. doi:10.1167/iovs.12-10565. PMID:22969068.
Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optometry and vision science : official publication of the American Academy of Optometry. 2019;96(8):556-567. doi:10.1097/OPX.0000000000001410. PMID:31343513.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.