Lacrimal canaliculus obstruction is a condition in which the lacrimal canaliculus (upper or lower canaliculus; vertical portion about 2 mm + horizontal portion about 8 mm = total about 10 mm) or the common canaliculus (from the junction of the upper and lower canaliculi to the entrance of the lacrimal sac) is blocked. Main causes include inflammatory scarring and postoperative adhesions.
Unilateral obstruction of one canaliculus often does not cause epiphora. In contrast, common canaliculus obstruction or bilateral canalicular obstruction prevents tear drainage into the nasolacrimal duct, resulting in significant epiphora. Prognosis depends largely on the extent of obstruction and the degree of scarring.
Anatomically, the upper and lower canaliculi run from the medial canthus nasally, bypass the Horner muscle, join at the common canaliculus, and open into the lacrimal sac. Understanding this anatomical pathway is crucial for diagnosis and treatment strategy.
It has been reported to occur after epidemic keratoconjunctivitis (EKC)1), and a multicenter study showed that about 60% of anticancer drug-related lacrimal duct obstructions involve punctum and canaliculus damage2).
QHow is lacrimal canaliculus obstruction different from nasolacrimal duct obstruction?
Lacrimal duct obstruction caused by S-1 (tegafur, gimeracil, oteracil potassium combination) often becomes severe. Among anticancer drug-related lacrimal duct obstructions, punctum and canaliculus disorders account for approximately 60%2), and the longer the time from onset of tearing symptoms, the more refractory it becomes. Note that obstruction may progress even after discontinuation of the drug.
QIf tearing occurs during use of S-1 (anticancer drug), how should it be managed?
A
Since lacrimal duct obstruction due to S-1 tends to become severe, early ophthalmologic consultation and consideration of tube intubation are recommended when tearing occurs. During anticancer drug use, tube removal may lead to re-obstruction, so it is desirable to continue tube placement while the drug is being used. Collaboration between the primary physician (oncologist) and ophthalmologist is important.
Detailed prevalence data for lacrimal canalicular obstruction are limited, but associations with the following diseases and conditions have been reported.
Lacrimal duct disorders after SJS often involve canalicular obstruction, and severe cicatricial obstruction tends to be difficult to treat. Acquired lacrimal duct obstruction after EKC (epidemic keratoconjunctivitis) has been reported relatively frequently in East Asia1).
Multicenter studies have reported lacrimal duct disorders in patients using S-1 2). Additionally, lacrimal sac biopsies performed during DCR (dacryocystorhinostomy) for lacrimal duct obstruction revealed granulation/reactive lymphoid hyperplasia in 5.9% and tumors in 1.4% (of which 69% were malignant) 3). Therefore, it is important to rule out neoplastic lesions in the differential diagnosis of epiphora and lacrimal duct obstruction.
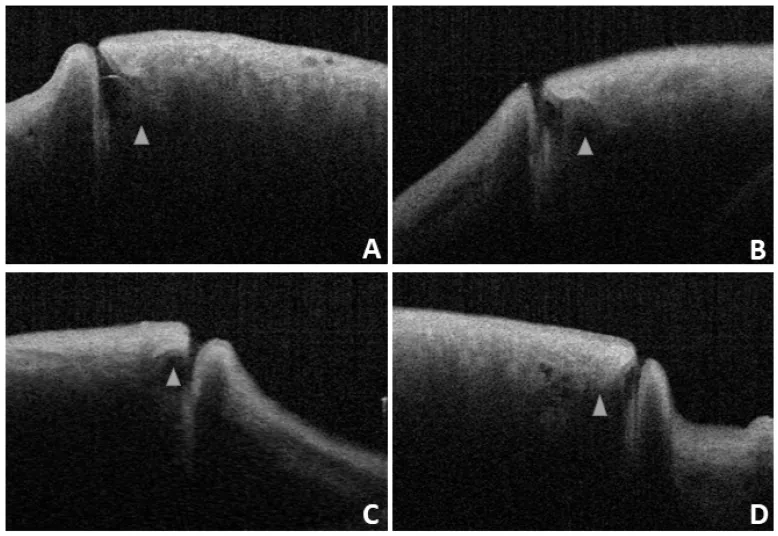
Hu J, Xiang N, Li GG, et al. Imaging and anatomical parameters of the lacrimal punctum and vertical canaliculus using optical coherence tomography. Int J Med Sci. 2021;18(12):2493-2499. Figure 4. PMID: 34104080; PMCID: PMC8176177; DOI: 10.7150/ijms.58291. License: CC BY.
Anterior segment OCT cross-sectional images of the lacrimal punctum and vertical canaliculus (ampulla) (A–D: 4 eyes). Triangles indicate the ampulla, and the lumen of the vertical part is visible. This corresponds to the anatomical evaluation of the lacrimal canaliculus (vertical part approximately 2 mm, horizontal part approximately 8 mm) discussed in the “Diagnosis and Examination Methods” section.
Check for patency of irrigation from each upper and lower punctum. Irrigation is the first step in estimating the site of obstruction, but its concordance rate with actual dacryoendoscopic findings is approximately 70% 1). The presence of reflux or resistance during irrigation provides diagnostic clues.
Considering the length of the lacrimal canaliculus (approximately 10 mm), estimate the extent of obstruction from the insertion length of the probe. In cases of common canalicular obstruction, inserting a metal probe yields a membranous resistance just before the lacrimal sac. Metal probes can easily create false passages, so they must be handled with particular care.
Dacryoendoscopy, which was covered by insurance in 2018 1), allows direct visualization of the obstruction site and is extremely useful for diagnosis. It can also assess the degree of fibrosis and mucosal inflammation at the obstruction site. It enables classification not only into common canalicular or nasolacrimal duct obstruction but also into detailed locations within the nasolacrimal duct 1).
The specifications of the scopes used are as follows:
Outer diameter 0.9 mm (observation pixel count 10,000 pixels)
Outer diameter 0.7 mm (3,000 pixels, prioritizing maneuverability)
2020 improved model: focal depth improved to 1.5–7 mm
Bent type (bends upward 27° at 10 mm from the tip) is mainly used
Dacryocystography is useful for identifying the site of obstruction and assessing the condition of the lacrimal sac, but it can be difficult to determine whether the contrast agent has reached the obstruction site 1). CT/MRI is recommended to rule out extralacrimal pathology and confirm bony obstruction 1, 4).
Perform intralacrimal anesthesia using 4% lidocaine hydrochloride solution. If the effect is insufficient, add infratrochlear nerve block (first branch of the trigeminal nerve) and intraorbital infiltration anesthesia with 2% lidocaine1).
Procedure
After sufficiently dilating the canaliculus with a punctum dilator, insert a nunchaku-type silicone tube or a catheter-type tube. During insertion, carefully check the sensation at the obstruction site and advance the tip little by little; do not force it. In some cases, the stenotic lacrimal passage may be dilated in advance with a bougie. Metal bougies are prone to creating false passages and must be handled with particular care.
The inserted tube is left in place for 1 to 2 months and then removed (for Grade 1, it may be longer, 2 to 10 months1)). If the tube is left in place for 9 months or longer, complications such as cheese-wiring (pressure erosion at the punctum) have been reported1), so caution is needed for long-term placement.
Probing using a lacrimal endoscope allows safe perforation of the obstruction under direct visualization1).
DEP (direct endoscopic probing): The lacrimal endoscope probe itself is used as a bougie to perforate the obstruction1).
SEP (sheath-guided endoscopic probing): A method of perforating with the tip of a Teflon lacrimal sheath. Perforation can be performed while observing the lumen1).
SGI (sheath-guided intubation): The tube is guided into the nasal cavity using the sheath as a guide. This significantly reduces submucosal misinsertion (approximately 22%) caused by blind insertion1).
G-SGI: A modification of SGI that eliminates the need for intranasal manipulation1).
Treatment outcomes for Grade 1: The Kaplan-Meier survival rate at a mean of 878.3 days postoperatively is 94%1), indicating a favorable prognosis. The reocclusion rate for canalicular obstruction is reported to be approximately 0–18.2%1).
If perforation is possible with DEP/SEP, tube insertion is performed similarly. When the obstruction is long, the lacrimal endoscopic image may show a continuous white wall-like appearance. Do not push with excessive force; instead, leave the sheath in place and attempt perforation by probing with a thin bougie, using any depressions or pits as a guide.
If the lacrimal endoscopic view appears yellowish, it indicates that the sub-mucosal orbital fat is visible, posing a risk of eyelid edema. If eyelid edema occurs, surgery should be discontinued. If only one side can be opened, a unilateral lacrimal tube is placed.
In patients using anticancer agents, reocclusion is likely after tube removal, so it is advisable to maintain tube placement while the medication is continued2).
5-4. Skin Incision Approach (Common Canalicular Obstruction Not Amenable to Punctal Perforation)
For common canalicular obstruction that cannot be perforated from the punctum, a skin incision approach is used.
Make a skin incision approximately 15–20 mm along the anterior lacrimal crest
Dissect the orbicularis oculi muscle over the lacrimal sac and incise the lacrimal sac
The location of the common punctum is estimated at the level of the medial canthal tendon
Insert a straight bougie from the punctum and, under direct microscopic visualization, confirm the position of the common punctum and perforate the obstructed area
Place a silicone tube threaded with a nylon suture in a ring shape through the upper and lower canaliculi
CDCR is indicated for cases where both the upper and lower canaliculi cannot be opened.
Jones tube method
The Jones tube is a glass tube that completely bypasses the lacrimal canaliculi to drain tears from the conjunctival sac into the nasal cavity. A report indicates that 87% of patients experienced therapeutic benefit5). Lifelong placement is required, and repositioning due to displacement or replacement due to clogging may occur. As of 2023, the Jones tube is not approved in Japan, limiting its use1). The first use of the Jones tube in Japan was reported by Nakagawa et al. in 19695).
QWhat is a Jones tube?
A
The Jones tube is a glass tube that completely bypasses the lacrimal canaliculi to drain tears from the conjunctival sac into the nasal cavity. It is used in cases where both the upper and lower lacrimal canaliculi are non-canalizable (CDCR-indicated cases). A report indicates that 87% of patients experienced therapeutic benefit. Lifelong placement is required, and repositioning or replacement due to displacement or clogging may be necessary. As of 2023, it is not approved in Japan, limiting its use.
Conjunctival pedicle flap method
The success rate is reported to be 75%5). This method involves temporary placement of a silicone sponge used in retinal detachment surgery, but the procedure is complex and may cause abduction limitation of the eye.
Endonasal CDCR
An endonasal method using a conjunctival pedicle flap has also been reported5). Similar to the external approach, there is a risk of abduction limitation.
This is a recently reported surgical technique that uses the lacrimal sac and nasolacrimal duct as a substitute for obstructed lacrimal canaliculi, directly anastomosing the lacrimal sac to the conjunctival sac6). Improvement of epiphora was confirmed in all 11 cases at one year postoperatively, with no complications reported6). It is expected as an alternative to CDCR, but long-term results are awaited.
Requires lifelong placement. Not approved in Japan
CDCR (conjunctival pedicle flap)
Same as above
75%5)
Risk of abduction deficit
Dacryocyst transposition
Same as above
100% (11 cases)6)
Awaiting accumulation of long-term results
QCan the lacrimal canaliculus become re-occluded after surgery for obstruction?
A
The re-occlusion rate after surgery for lacrimal canalicular obstruction is reported to be approximately 0–18.2%. For Grade 1, the Kaplan-Meier survival rate is 94% (mean follow-up 878.3 days), which is favorable, but re-occlusion can occur even after initial patency is achieved. The risk is higher when the causative disease (e.g., SJS) remains active or when the obstruction is long. The survival rate at 3,000 days postoperatively is reported to be 64%, so long-term follow-up with consideration of recurrence risk is necessary.
The lumen of the lacrimal canaliculus is lined by non-keratinized stratified squamous epithelium, which functions in the passage of tear components and defense. The lacrimal canaliculus consists of a vertical portion (approximately 2 mm) and a horizontal portion (approximately 8 mm), with a total length of about 10 mm. The upper and lower canaliculi join via Horner’s muscle (posterior limb of the medial canthal tendon) to form the common canaliculus (approximately 2–5 mm long), which opens into the lacrimal sac.
Mechanism of Inflammatory and Cicatricial Obstruction
Tegafur (the main component of S-1) is metabolized in the body to 5-FU (fluorouracil). 5-FU is secreted into tears and directly damages the epithelial cells of the lacrimal duct mucosa, causing lacrimal canalicular obstruction. The risk increases with dose and duration of administration, and obstruction may progress even after the onset of epiphora symptoms.
Anatomical Background of Common Canalicular Obstruction
The common canaliculus is located at the height of the medial canthal tendon and is approachable from the skin side. This anatomical relationship provides the theoretical basis for perforation via a skin incision. When the obstruction is long or scarring is severe, surgical reconstruction is extremely difficult, and bypass procedures such as CDCR or dacryocyst transposition become options.
Dacryocyst transposition is a recently reported surgical technique6) and is expected to be an alternative to CDCR. At one year postoperatively, all 11 cases showed improvement in epiphora, with no reported complications. Accumulation of long-term outcomes and comparison with CDCR remain future challenges.
Lacrimal endoscopy has been continuously improved from the early model (6,000 pixels) in 2002 to 2012 (10,000 pixels) and 2020 (improved depth of focus to 1.5–7 mm), enabling more detailed observation of the obstruction site. The spread of SGI and G-SGI has reduced the risk of submucosal misinsertion1), and standardization of the procedure is expected in the future.
Furthermore, establishing a method to determine the optimal timing for tube removal based on lacrimal endoscopic findings is thought to improve postoperative outcomes1).
The survival rate at 3,000 days after tube removal has been reported as 64%6). This suggests the need for long-term follow-up, and regular postoperative lacrimal irrigation tests are important for monitoring.
Kashkouli MB, Pakdel F, Kiavash V. Assessment and management of proximal and incomplete symptomatic obstruction of the lacrimal drainage system. Middle East Afr J Ophthalmol. 2012;19(1):60-9. doi:10.4103/0974-9233.92117. PMID:22346116. PMCID:PMC3277026.
Kim Y, Lew H. Dacryoendoscopic Findings of Patients with Lacrimal Drainage Obstruction Associated with Cancer Treatment. Korean J Ophthalmol. 2022;36(6):509-517. doi:10.3341/kjo.2022.0051. PMID: 36220641; PMCID: PMC9745344.
Koturović Z, Knežević M, Rašić DM. Clinical significance of routine lacrimal sac biopsy during dacryocystorhinostomy: a comprehensive review of literature. Bosn J Basic Med Sci. 2017;17(1):1-8. doi:10.17305/bjbms.2016.1424. https://doi.org/10.17305/bjbms.2016.1424
辻英貴. 涙道にみられる腫瘍の診断と治療. 眼科手術. 2022;35(2):247-251.
Chang M, Lee H, Park M, Baek S. Long-term outcomes of endoscopic endonasal conjunctivodacryocystorhinostomy with Jones tube placement: a thirteen-year experience. J Craniomaxillofac Surg. 2015;43(1):7-10. doi:10.1016/j.jcms.2014.10.001. PMID:25459376.
Sugimoto M. Dacryoendoscopy as a frontier technology for lacrimal drainage disorders. Jpn J Ophthalmol. 2025. doi:10.1007/s10384-025-01255-7. https://doi.org/10.1007/s10384-025-01255-7
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.