
Lacrimal Endoscopy
1. What is dacryoendoscopy?
Section titled “1. What is dacryoendoscopy?”Dacryoendoscopy / lacrimal endoscopy is a test in which a thin optical endoscope with an outer diameter of 0.7–0.9 mm is inserted from the punctum and used to directly observe the lumen of the lacrimal drainage system (canaliculus, common canaliculus, lacrimal sac, and nasolacrimal duct). It can provide information on lesions within the lacrimal passage, the degree of obstruction, and the postoperative condition of the lacrimal mucosa1).
It was developed in Japan by Suzuki and colleagues in 20021) and has since been improved. It was covered by insurance in 2018 and is now widely used in outpatient clinics and operating rooms as a standard tool for lacrimal care.
Types of devices and features
Section titled “Types of devices and features”There are two types of devices available in Japan: those made by Fibertech and those made by Machida Manufacturing. The bent type, which bends upward by 27° at a point 10 mm from the tip, is the most common, but straight and double-bent types are also used depending on the case.
The number of observation pixels was 6,000 at the time of development (2002), but in 2012 it was improved to 10,000 while keeping the outer diameter at 0.9 mm. In 2020, improvements to the tip lens increased the observation distance to 1.5–7 mm, dramatically improving depth of focus1).
It was covered by insurance in 2018. Before that, many facilities offered it only as self-pay care, but since coverage it has become widely used as a standard method for confirming lacrimal duct obstruction and for preoperative evaluation.
2. Device specifications
Section titled “2. Device specifications”Lacrimal endoscopes come in standard and small-diameter types, and each has a different use.
| Specification item | Standard type | Small-diameter type |
|---|---|---|
| Tip outer diameter | 0.9 mm | 0.7 mm |
| Observation pixels | 10,000 | 3,000 |
| Main uses | Detailed observation / identification of the blockage site | Emphasis on maneuverability / narrow lacrimal ducts |
The standard type (outer diameter 0.9 mm) has a high imaging pixel count and can show the fine structure of the mucosa, the course of blood vessels, and the shape of masses in detail. The small-diameter type (outer diameter 0.7 mm) has a thinner tip and is easier to handle in cases with a narrow punctum or a deformed canaliculus.
The endoscope is equipped with an irrigation channel and a light source, allowing saline to be infused and suctioned while observing. The bent type has an upward 27° bend 10 mm from the tip, making it possible to change direction from the lacrimal sac to the nasolacrimal duct with smooth handling.
3. Indications
Section titled “3. Indications”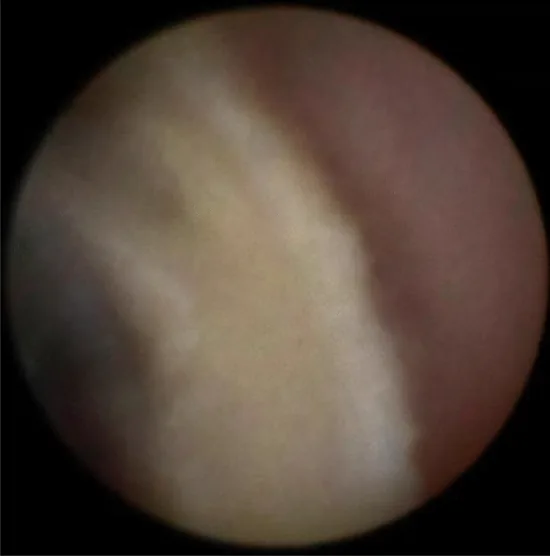
Lacrimal endoscopy is excellent for observing the inside of the lacrimal drainage system, but it is not suited to understanding the anatomical relationship with the surrounding tissues. Therefore, when needed, it is used together with CT and MRI1).
The main indications are as follows.
- Confirming the site and extent of lacrimal duct obstruction — The concordance rate with the irrigation test is around 70%1). Used for definitive diagnosis in cases where obstruction is suspected on irrigation testing
- Early detection of masses in the lacrimal duct — Observation of malignant melanoma, papilloma, and granuloma. In pathology at the time of DCR, tumors were detected in 1.4%, of which 69% were malignant1)
- Confirmation of lacrimal duct stones in canaliculitis and confirmation of their removal — White, clump-like stones can be directly seen
- Diagnosis of lacrimal sac stones — Lacrimal sac stones have been reported in 7.5% of cases of nasolacrimal duct obstruction1)
- Postoperative follow-up and investigation of causes in poorly recovering cases — Checking the mucosal condition and the mechanism of re-obstruction after lacrimal tube placement
- Diagnosis of displaced punctal plugs — Migration into the canaliculus can be directly confirmed
The irrigation test is simple and can be performed immediately in the outpatient clinic, but its accuracy for estimating the site of obstruction matches lacrimal endoscopy findings only at about 70%1). Lacrimal endoscopy allows direct observation of the lacrimal passage lumen and can evaluate the exact site and degree of obstruction, the mucosal condition, and whether a mass is present. These two tests complement each other, and it is common to perform lacrimal endoscopy for a detailed evaluation when irrigation suggests obstruction.
4. Examination procedure (preoperative preparation, anesthesia, and insertion technique)
Section titled “4. Examination procedure (preoperative preparation, anesthesia, and insertion technique)”Preoperative examination and history taking
Section titled “Preoperative examination and history taking”During the history, confirm any prior treatment for sinusitis, a history of epidemic keratoconjunctivitis (EKC), a history of facial trauma, medication use (fluoropyrimidine anticancer drugs such as TS-1 and Rebamipide eye drops), and whether the patient uses pools. These are helpful for estimating the cause of lacrimal duct disease1).
The flow of the preoperative examination is shown below.
- History taking — Confirm the items above
- Slit-lamp examination — Evaluate the nature of the tears, the shape of the punctum, the conjunctiva, and the cornea
- Palpation around the lacrimal sac — check for swelling, induration, and tenderness
- Lacrimal sac irrigation (syringing test) — assess the presence and degree of obstruction in advance
- Blood tests — liver and kidney function, complete blood count, and coagulation tests (when a surgical procedure will be performed)
If the patient has cardiovascular disease, assess the overall condition individually and decide whether the procedure can be performed.
Anesthesia methods
Section titled “Anesthesia methods”In adults, the procedure can be performed under local anesthesia.
- Basic anesthesia (observation only): topical oxybuprocaine hydrochloride + topical 4% lidocaine + mucosal anesthesia of the lacrimal drainage system by instilling 4% lidocaine into the lacrimal passage1)
- Additional anesthesia (when opening an obstruction or inserting a tube): add an infratrochlear nerve (a branch of the first division of the trigeminal nerve) block using 2% lidocaine + infiltration anesthesia into the orbital tissues1)
For infratrochlear nerve anesthesia, when using a 19 mm needle, a guideline is to insert the needle about one-half to two-thirds of its length. Do not use epinephrine-containing medications in the orbit because of the risk of ophthalmic artery constriction1).
In infants and young children, general anesthesia is often chosen.
Positioning
Section titled “Positioning”Adjust the patient to a supine position with the head level. Keep the tip of the nose facing upward and the chin not elevated. An improper head position can lead to forceful manipulation of the lacrimal endoscope and increase the risk of injury1).
Punctal dilation and endoscope insertion
Section titled “Punctal dilation and endoscope insertion”- Punctal dilation: For an endoscope outer diameter of φ0.9 mm, a dilation diameter of about φ1.0 mm is the guideline. Use a punctal dilator to widen it gently.
- Eyelid traction: Pull the eyelid firmly outward to straighten the horizontal portion of the canaliculus. If straightening is insufficient, the tip can touch the canalicular side wall and create false resistance.
- Insertion into the canaliculus: The canaliculus runs vertically for about 2 mm from the punctum, then bends at nearly a right angle toward the lacrimal sac. Insert with this anatomy in mind. From the upper punctum, the lacrimal sac can be reached almost straight.
- Observation inside the lacrimal sac: Once you pass the common canaliculus and reach the lacrimal sac, the vascular pattern of the inner wall (orange-red mucosa) becomes visible.
- Exploring the nasolacrimal duct: Rotate the tip so it points downward, and look for the entrance to the nasolacrimal duct. The valve of Hasner often opens on the nasal side.
5. Normal and abnormal findings
Section titled “5. Normal and abnormal findings”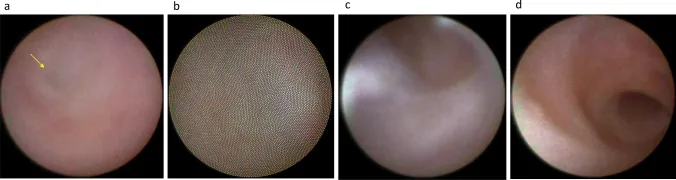
Normal lacrimal endoscopic findings
Section titled “Normal lacrimal endoscopic findings”It is essential to understand the normal findings at each site in order to recognize abnormal findings.
- Canaliculus: Mucosa with strong white reflections. Shows a white sheen without inflammation or fibrosis
- Lacrimal sac: Orange-red mucosa with visible blood vessels. The vascular pattern appears normal
- Nasolacrimal duct: A curved lumen continues, and the valve of Hasner opens on the nasal side
- Entire lacrimal duct mucosa: No signs of inflammation, no mass, no stones
Typical abnormal findings
Section titled “Typical abnormal findings”| Finding | Clinical significance |
|---|---|
| White fibrotic mucosa | Useful for identifying the site of obstruction (lower nasolacrimal duct vs common canaliculus) |
| Raised lesion | Suspicion of papilloma, granuloma, or malignant tumor — consider biopsy |
| White mass-like material (stone) | Used to confirm canaliculitis and lacrimal sac stones — also used to confirm removal |
| Mucosal redness and inflammatory findings | Diagnosis of active lacrimal duct inflammation |
| Black-to-gray lesion | Suspected melanoma — note that it may appear gray because of auto exposure |
When a black object is observed with a lacrimal endoscope, the camera’s auto-exposure mode may render it gray rather than black. When observing melanoma, keep this in mind and do not judge benign or malignant based on color alone1).
Masses can occur inside the lacrimal passage, and pathological examination during dacryocystorhinostomy (DCR) detected tumors in 1.4%. In addition, 69% of those were reported to be malignant tumors1), and delayed detection can affect prognosis. Lacrimal endoscopy is useful for early detection of masses, and if an elevated lesion is seen, it is important to perform biopsy and pathological examination.
6. Treatment applications (DEP・SEP・SGI)
Section titled “6. Treatment applications (DEP・SEP・SGI)”Lacrimal endoscopy is notable in that it can be used not only for examination but also for transendoscopic recanalization (endoscopic lacrimal ductoplasty).
- DEP (direct endoscopic probing): A method that uses the probe tip itself as a bougie to pierce the obstruction. The simplest procedure
- SEP (sheath-guided endoscopic probing): A method that uses a Teflon sheath as an outer tube and pierces the obstruction under endoscopic guidance. Because the sheath stabilizes the obstruction site, penetration is more stable
- SGI (sheath-guided intubation): After SEP, the sheath is left in place and a lacrimal tube is inserted into the sheath and guided to the nasal cavity. This can greatly reduce submucosal misinsertion (false passage), which occurred in 22% with the conventional method1)
By using these procedures appropriately, lacrimal reconstruction can be performed according to the degree and site of obstruction and the mucosal condition. Combining lacrimal tube intubation with lacrimal endoscopy allows a single, integrated procedure through postoperative irrigation confirmation and evaluation of the mucosal condition.
7. Disinfection, Complications, and Precautions
Section titled “7. Disinfection, Complications, and Precautions”Disinfection and Infection Control
Section titled “Disinfection and Infection Control”Because the lacrimal passages are continuous with the nasal cavity, it is difficult to maintain a completely sterile state, but every effort should be made to sterilize as much as possible1).
- Povidone-iodine disinfection around the eyelids
- Iodine eye drops
- The endoscope itself should undergo proper disinfection and sterilization before and after use
Precautions for Device Management
Section titled “Precautions for Device Management”The base of the lacrimal endoscope probe (near the connector) is a fragile area and requires careful handling1). Bending or excessive twisting can lead to wire breakage, so avoid forcing the instrument during insertion and removal.
Precautions Regarding Anesthesia
Section titled “Precautions Regarding Anesthesia”- Epinephrine-containing medications for the orbit: Avoid use because of the risk of ophthalmic artery narrowing1)
- Complications of infratrochlear nerve anesthesia: There is a risk of retrobulbar hemorrhage. Complete avoidance is not possible, so explain this to the patient before the procedure and obtain consent1)
- Infants and young children: Because it is difficult to control movement with local anesthesia, the procedure is generally performed under general anesthesia
Points to note in differential diagnosis and interpretation
Section titled “Points to note in differential diagnosis and interpretation”- Black lesions may appear gray because of auto-exposure, so do not rule out malignancy based on color alone1)
- Lacrimal endoscopy is excellent for evaluating the lacrimal duct lumen, but it should be combined with CT and MRI to understand the surrounding structures (inside the orbit and the paranasal sinuses)1)
- The agreement rate with the irrigation test is around 70%, and even when the irrigation test is “good,” the endoscopic view may still show mucosal changes1)
8. References
Section titled “8. References”- 日本涙道・涙液学会涙道内視鏡診療の手引き作成委員会. 涙道内視鏡診療の手引き. 日本眼科学会雑誌. 2023;127(10):896-917.