
Semaglutide and Related Ocular Risks
Key points at a glance
Section titled “Key points at a glance”1. Ocular risks associated with semaglutide
Section titled “1. Ocular risks associated with semaglutide”Semaglutide is a GLP-1 receptor agonist (GLP-1RA) that promotes insulin secretion in response to hyperglycemia and lowers blood glucose levels. It was FDA-approved for the treatment of type 2 diabetes (T2DM) as Ozempic in December 2017, and as a weight loss drug, Wegovy, in December 2022. From 2021 to 2023, weekly GLP-1RA prescriptions in the United States increased by approximately 60%, and with this expanded use, interest in ocular side effects has grown.
The main reported ocular risks are the following two.
- Worsening of diabetic retinopathy (DR): May occur as early worsening due to rapid blood glucose lowering.
- Non-arteritic anterior ischemic optic neuropathy (NAION): A disease that causes acute, painless vision loss due to reduced blood flow to the optic disc, and is the most common form of ischemic optic neuropathy. The estimated annual incidence of NAION is 2.3 to 10.2 per 100,000 people aged 50 and older3), and there is no effective treatment, with more than half of patients not experiencing visual improvement after the acute phase.3)
Macular edema has also been reported as a related finding, but it often occurs in the context of worsening diabetic retinopathy.
Two main complications have been reported: non-arteritic anterior ischemic optic neuropathy (NAION) and worsening of diabetic retinopathy. Macular edema is also listed as a related finding. None of these have a confirmed causal relationship, and conclusions vary by study, especially for NAION.
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”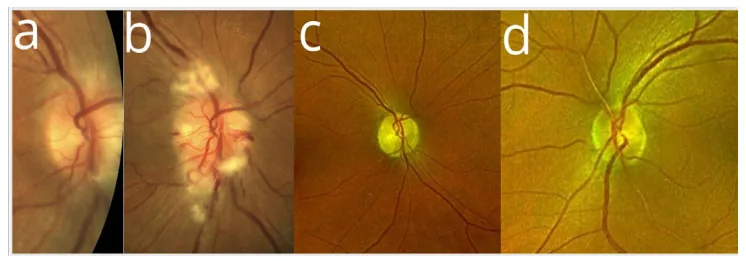
Subjective Symptoms
Section titled “Subjective Symptoms”- Acute, painless vision loss (related to non-arteritic anterior ischemic optic neuropathy): Sudden onset in one eye. Non-arteritic anterior ischemic optic neuropathy is usually painless.
- Vision loss and floaters (related to worsening diabetic retinopathy): Occurs when pre-existing retinopathy progresses after starting semaglutide. Vitreous hemorrhage may cause floaters.
- Decreased central vision and distortion (related to macular edema): Macular edema associated with worsening diabetic retinopathy leads to decreased central vision and metamorphopsia.
Clinical Findings
Section titled “Clinical Findings”- Optic disc edema (acute phase of non-arteritic anterior ischemic optic neuropathy): Disc edema is observed in the acute phase. It progresses to optic atrophy in the chronic phase. Accompanied by visual field defects.
- Proliferative diabetic retinopathy progression (DR worsening): Appearance of new blood vessels, vitreous hemorrhage, tractional retinal detachment, etc.
- Macular edema: Edema occurs in the macula with worsening DR.
In the SUSTAIN-6 trial, the semaglutide group had a significantly higher risk of retinopathy-related complications (blindness, vitreous hemorrhage, need for photocoagulation, use of intravitreal injections) compared to the placebo group (HR 1.76; 95% CI, 1.11–2.78; P = 0.02). 4)
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Mechanism of DR worsening by semaglutide (presumed)
Section titled “Mechanism of DR worsening by semaglutide (presumed)”- Rapid blood glucose lowering (early worsening): A rapid decrease in HbA1c may temporarily worsen existing retinopathy. This is a known phenomenon with strict glycemic control (DCCT trial), and a similar mechanism is thought to occur with semaglutide.
Risk factors for DR worsening
Section titled “Risk factors for DR worsening”In a meta-analysis of 23 RCTs (22,096 patients), the risk ratio for DR development in the semaglutide group was RR 1.24 (95% CI, 1.03–1.50) compared with placebo. 4)
The risk of DR worsening is particularly high in the following patients:
- Pre-existing diabetic retinopathy (especially severe cases)
- Age 60 years or older (RR 1.27; 95% CI, 1.02–1.59) 4)
- Diabetes duration of 10 years or more (RR 1.28; 95% CI, 1.04–1.58) 4)
Common risk factors for non-arteritic anterior ischemic optic neuropathy
Section titled “Common risk factors for non-arteritic anterior ischemic optic neuropathy”- Small cup-to-disc ratio (crowded disc): The strongest risk factor for non-arteritic anterior ischemic optic neuropathy, considered more important than systemic risk factors such as diabetes. 2)
- Hypertension, hyperlipidemia, diabetes, obstructive sleep apnea
- Medications that may increase risk: amiodarone, phosphodiesterase inhibitors 3)
Hypothesis of the association between semaglutide and non-arteritic anterior ischemic optic neuropathy
Section titled “Hypothesis of the association between semaglutide and non-arteritic anterior ischemic optic neuropathy”Although a causal relationship has not been established, the following hypothesis has been proposed.
- GLP-1RAs may affect vascular dynamics via the autonomic nervous system, reducing systemic blood pressure and potentially influencing optic disc perfusion2)
- GLP-1 receptors exist in the human optic nerve, and sympathetic hyperactivity induced by GLP-1RAs may increase susceptibility to non-arteritic anterior ischemic optic neuropathy
- On the other hand, GLP-1RAs have also been reported to have neuroprotective and ischemia risk-reducing effects, and the mechanism remains unclear2)
Non-arteritic anterior ischemic optic neuropathy is a rare disease (about 14.5 per 100,000 person-years), and not all patients using semaglutide develop it. Multiple large studies show a small increase in risk, and some studies did not find a significant difference. It has been suggested that the benefits of semaglutide in blood glucose control and cardiovascular protection may outweigh the potential risk of non-arteritic anterior ischemic optic neuropathy. 3)
4. Diagnosis and Testing Methods
Section titled “4. Diagnosis and Testing Methods”In patients using semaglutide, the following monitoring and evaluation are important.
Pre-treatment Evaluation
Section titled “Pre-treatment Evaluation”- Dilated fundus examination: Consider performing before starting semaglutide to diagnose and treat ocular complications such as diabetic retinopathy (DR) simultaneously.
- DR screening at T2DM diagnosis: Perform fundus examination at the time of T2DM diagnosis to check for the presence of existing retinopathy.
Monitoring During Treatment
Section titled “Monitoring During Treatment”- Regular fundus examination: After starting semaglutide, especially in patients with existing DR, perform regular examinations for early detection of DR worsening. Continue annual screening after T2DM diagnosis.
- If non-arteritic anterior ischemic optic neuropathy is suspected: Perform visual acuity test, visual field test, fundus examination (to check for optic disc edema), and fluorescein angiography.
5. Clinical Recommendations
Section titled “5. Clinical Recommendations”DR-Related Recommendations
Section titled “DR-Related Recommendations”- Perform dilated fundus examination before initiating semaglutide therapy, and simultaneously diagnose and treat any coexisting DR.
- Consider reducing insulin therapy or discontinuing sulfonylureas to reduce the risk of rapid DR worsening.
- In severe DR, initiate retinopathy treatment before or concurrently with glucose-lowering therapy (transient worsening is expected).
- Apply DR management guidelines similarly to patients using other diabetes medications (e.g., anti-VEGF agents, retinal photocoagulation).
Recommendations related to non-arteritic anterior ischemic optic neuropathy
Section titled “Recommendations related to non-arteritic anterior ischemic optic neuropathy”- For patients with a history of or risk factors for non-arteritic anterior ischemic optic neuropathy, provide thorough prior explanation about the possible association between semaglutide and vision loss.
- A cautious approach is necessary in cases with concomitant insulin therapy or disease progression.
It is recommended to perform a dilated fundus examination before starting semaglutide. If pre-existing diabetic retinopathy (DR) is present, diagnosis and treatment should be performed simultaneously. If severe DR is present, consider initiating retinopathy treatment in parallel with glucose-lowering therapy. Screening for DR at the time of T2DM diagnosis and annually thereafter is also important.
6. Pathophysiology and Detailed Mechanisms
Section titled “6. Pathophysiology and Detailed Mechanisms”Pharmacological Effects of Semaglutide
Section titled “Pharmacological Effects of Semaglutide”Semaglutide is a long-acting GLP-1 receptor agonist.
- Stimulates insulin secretion in response to high blood glucose.
- Suppresses glucagon release and reduces hepatic gluconeogenesis, thereby lowering blood glucose levels.
- Promotes weight loss through delayed gastric emptying and reduction of hunger and food cravings.
- Resists rapid degradation by DPP-4, providing sustained therapeutic effects.
Mechanism of DR Worsening
Section titled “Mechanism of DR Worsening”The main mechanism of DR worsening is early worsening associated with rapid blood glucose reduction.
- In the SUSTAIN-6 trial, semaglutide was associated with a HR of 1.76 (95% CI, 1.11–2.78) for retinopathy-related complications. 4)
- A meta-analysis of 23 RCTs (22,096 patients) showed a RR of 1.24 (95% CI, 1.03–1.50) for retinopathy development with semaglutide vs placebo. 4)
- Rapid reduction in HbA1c is presumed to cause functional and structural changes in existing retinal vessels, but the detailed mechanism remains unclear.
Pathophysiological hypothesis of the association with non-arteritic anterior ischemic optic neuropathy
Section titled “Pathophysiological hypothesis of the association with non-arteritic anterior ischemic optic neuropathy”Non-arteritic anterior ischemic optic neuropathy is a multifactorial disease, resulting from a combination of vascular factors (optic disc hypoperfusion) and anatomical factors (small cup-to-disc ratio, optic disc drusen). 3)
- GLP-1RAs may affect vascular dynamics via the autonomic nervous system, potentially leading to reduced systemic blood pressure and subsequent effects on optic disc perfusion. 2)
- Semaglutide has a stroke prevention effect (SUSTAIN 6 + PIONEER 6 pooled analysis) and is considered effective against small vessel occlusion. 3)
- However, there is no known mechanistic link between GLP-1RAs and nonarteritic anterior ischemic optic neuropathy 2), and neuroprotective effects and ischemic risk reduction have also been reported, so the involvement in the development of nonarteritic anterior ischemic optic neuropathy is unclear.
7. Latest Research and Future Perspectives (Research-Stage Reports)
Section titled “7. Latest Research and Future Perspectives (Research-Stage Reports)”Three major studies have examined the association between semaglutide and nonarteritic anterior ischemic optic neuropathy, but their conclusions are inconsistent. The following is a summary of each study.
Hathaway JT et al. (2024) reported a retrospective matched cohort study at Massachusetts Eye and Ear (December 2017 to November 2023)1). In the T2D group (semaglutide n=194 vs non-GLP-1RA n=516), the 36-month cumulative incidence of nonarteritic anterior ischemic optic neuropathy was 8.9% (95% CI, 4.5%–13.1%) in the semaglutide group vs 1.8% (95% CI, 0%–3.5%) in the non-GLP-1RA group, HR 4.28 (95% CI, 1.62–11.29; P < .001). In the overweight/obesity group (semaglutide n=361 vs non-GLP-1RA n=618), a significant risk increase was also observed with HR 7.64 (95% CI, 2.21–26.36; P < .001). The risk was most pronounced within the first year after prescription, suggesting a possible drug-induced effect. However, this was a single-center, specialized facility study with limitations including unadjusted HbA1c, BMI, and insulin use.
Cai CX et al. (2025) reported a large retrospective study using the OHDSI 14 database (37 million T2D patients)2). The incidence of nonarteritic anterior ischemic optic neuropathy among new semaglutide users was 14.5 per 100,000 person-years (sensitive definition). Cohort analyses comparing semaglutide with other GLP-1RAs or non-GLP-1RA drugs showed no significant differences. Self-controlled case series (SCCS) analysis confirmed an increased risk of nonarteritic anterior ischemic optic neuropathy during semaglutide exposure (IRR 1.32; 95% CI, 1.14–1.54; P < .001, specific definition), but the risk was smaller than in the Hathaway study. No increased risk of nonarteritic anterior ischemic optic neuropathy was observed with dulaglutide, suggesting a possible semaglutide-specific effect.
Chou CC et al. (2025) reported a multinational population-based cohort study using TriNetX (21 countries, approximately 200 million people) 3). They divided participants into three groups (T2DM only, obesity only, T2DM+obesity; total >290,000) and found no significant increase in non-arteritic anterior ischemic optic neuropathy risk over up to 3 years of follow-up in any group (T2DM only group 3-year HR 1.51; 95% CI, 0.71–3.25). After adjusting for BMI, HbA1c, and insulin use, they concluded that semaglutide is not significantly associated with non-arteritic anterior ischemic optic neuropathy in the general population.
The results of the three studies are summarized below.
| Study | Sample size | Main result (NAION) | Conclusion |
|---|---|---|---|
| Hathaway 20241) | Single center, approximately 1,700 people | T2D group HR 4.28 | Significant increase in risk |
| Cai 20252) | OHDSI 37.1 million people | SCCS IRR 1.32 | Small increase in risk |
| Chou 20253) | TriNetX approximately 300,000 people | 3-year HR 1.51 (ns) | Not statistically significant |
Future challenges: Prospective cohort studies and clinical trials are needed to confirm causality.3) Studies including ophthalmic risk factors (e.g., cup-to-disc ratio) and evaluation of dose dependency are also important issues.2) Clinicians should weigh the risk of non-arteritic anterior ischemic optic neuropathy, a rare but potentially blinding disease, against the many therapeutic benefits of semaglutide.2)
Differences in study design are the main cause. The Hathaway study was a small cohort from a single specialized facility, raising concerns about selection bias. The Cai study used large-scale data from 37.1 million people but had limitations due to its self-controlled design. The Chou study is characterized by dividing the population into three groups and adjusting for BMI, HbA1c, and insulin use, with differences in confounder adjustment methods affecting the conclusions.
8. References
Section titled “8. References”- Hathaway JT, Shah MP, Hathaway DB, et al. Risk of Nonarteritic Anterior Ischemic Optic Neuropathy in Patients Prescribed Semaglutide. JAMA Ophthalmol. 2024;142(8):732-739.
- Cai CX, Mathioudakis N, Fan R, et al. Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy. JAMA Ophthalmol. 2025;143(4):304-314.
- Chou CC, Pan SY, Sheen YJ, et al. Association between Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy: A Multinational Population-Based Study. Ophthalmology. 2025;132(4):381-388.
- Lim JI, Kim SJ, Bailey ST, et al. Diabetic Retinopathy Preferred Practice Pattern. Ophthalmology. 2025 Apr;132(4):P75-P162. doi:10.1016/j.ophtha.2024.12.020. PMID:39918521.