LADA (Latent Autoimmune Diabetes in Adults) is a disease concept first reported as a subcategory of adult patients who have autoantibodies against GAD65 while exhibiting a T2DM phenotype. It is also called “type 1.5 diabetes.”
Diagnostic criteria (Japan Diabetes Society IDS) consist of the following three items.
Age at onset 30 years or older
At least one type of pancreatic islet autoantibody positive
Insulin independence for 6 months after diagnosis
The prevalence is 2–12% of all diabetes, and the rate of misdiagnosis as T2D is estimated at 5–10% 5). The discovery of islet cell antibodies (ICA) dates back to 1974 and greatly transformed the classification of diabetes.
From a neuro-ophthalmological perspective, chronic hyperglycemia-induced microvascular damage causes diabetic retinopathy, NAION (non-arteritic anterior ischemic optic neuropathy), homonymous hemianopia due to cortical stroke, oculomotor nerve palsy, nystagmus, and others. The prevalence of diabetic retinopathy in LADA patients is significantly lower than in T2D patients (20.3% vs 26.4%, P < 0.001). About 12% of cases have retinopathy at diagnosis.
QHow is LADA different from type 2 diabetes?
A
LADA is positive for autoantibodies and slowly progresses to insulin dependence, whereas T2D is negative for autoantibodies and remains insulin-independent for a long time. It is positioned as “type 1.5” sharing both genetic and clinical features of LADA and T2D.
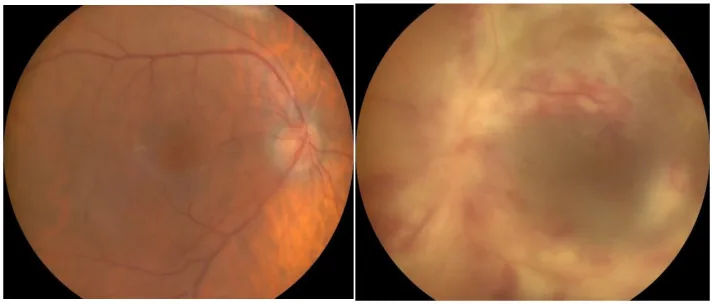
Emil Robert Stoicescu, Laura Andreea Ghenciu, Roxana Iacob et al. CMV Retinitis in the Context of SARS-CoV-2 Infection: A Case Study and Comprehensive Review of Viral Interactions. Pathogens. 2024 Oct 29; 13(11):938. Figure 1. PMCID: PMC11597558. License: CC BY.
Polyuria, polyphagia, polydipsia, dehydration: Systemic symptoms associated with hyperglycemia.
Visual symptoms: Visual impairment or visual field defects due to diabetic retinopathy, non-arteritic anterior ischemic optic neuropathy, or cortical stroke.
DKA symptoms: Seizures and coma associated with ketoacidosis (acute onset similar to T1D).
Small fiber neuropathy: Pain, burning sensation, and stinging starting from the feet. Caused by atrophy of Aδ and C fibers.
Diabetic papillopathy: optic disc swelling with microvascular dilation. May be accompanied by surrounding hemorrhages and white spots. RAPD is negative, visual field testing shows only enlarged blind spot. Spontaneous remission within 3–6 months.
Ischemic optic neuropathy: due to circulatory disturbance of the posterior ciliary arteries and branches of the central retinal artery.
Cortical stroke (homonymous hemianopia): occurs as a result of cerebrovascular disease due to chronic hyperglycemia.
Efferent Disorders
Ocular motor cranial nerve palsy: palsy of cranial nerves III, IV, and VI. Diabetic ophthalmoplegia most commonly involves the oculomotor nerve, followed by the abducens nerve; trochlear nerve palsy is rare. Most cases resolve spontaneously within a few months.
Pupillary abnormalities: In diabetes, there is a tendency toward miosis, and the pupil dilates poorly with mydriatic agents (sympathetic nerve disorder and dilator pupillae muscle disorder).
Nystagmus: Associated with GAD antibody-related neurological diseases (stiff-person syndrome and cerebellar ataxia).
Other ocular findings include the following.
Corneal abnormalities: Endothelial cell pleomorphism and Descemet membrane folds. If Descemet membrane folds are observed in individuals under 60 years of age, diabetes should be suspected.
Iridocyclitis: Often mild, with only cells in the anterior chamber, and resolves quickly with steroid eye drops.
Orbital mucormycosis: Occurs in patients with poor glycemic control. High mortality rate; treated with antifungal drugs.
Autoantibodies against pancreatic islet beta cells (GAD65, ICA, IA-2A, IAA) are produced, leading to beta cell destruction. The process leading to insulin deficiency involves a combination of mechanisms from both T1DM and T2DM.
COVID-19 related: SARS-CoV-2 may trigger autoimmune reactions against pancreatic β cells via ACE2 receptors. It has been reported that 20% of hospitalized COVID-19 patients acquired new autoantibodies after hospitalization1)
Obesity promoting factors: Even with GAD65-Ab positivity, some cases do not develop LADA for 3 years if BMI is stable, suggesting weight gain may promote LADA onset4)
QDoes COVID-19 infection increase the risk of developing LADA?
A
There are case reports of autoantibodies such as IA2 appearing after COVID-191). A mechanism of β-cell injury via ACE2 receptors has been proposed, but a causal relationship has not been established at this time.
For example, in a post-COVID-19 LADA case, the following test value pattern has been reported: GAD65 < 5 nmol/L (normal), C-peptide 2.38 ng/mL (normal), IA2 20.6 DK units/mL (high, normal < 5.4)1).
Slit-lamp examination: Check for corneal abnormalities and iridocyclitis
Dilated fundus examination: Check for microaneurysms, hemorrhages, exudates, edema, retinal neovascularization, vitreous cells, and retinal detachment around the macula
A comparison of each diabetes type is shown below.
Item
LADA
T1D
T2D
Age at onset
30 years or older
Mostly under 35 years
35 years or older
Autoantibodies
Positive
Often positive
Negative
C-peptide
Normal to low
Low
Normal to high
Insulin dependence
Slowly progressive
From onset
Long-term non-dependent
Other differential diagnoses include MODY (strong family history, negative autoantibodies) and LADY (slowly progressive autoimmune diabetes in young adults).
QWhich test is most important for diagnosing LADA?
A
The combination of GAD65 antibody (highest sensitivity) and C-peptide testing is most important for diagnosis. Low C-peptide levels with positive autoantibodies confirm LADA. The IDS classification criteria (age at onset ≥30 years, positive autoantibodies, insulin independence for 6 months after diagnosis) are also used for diagnosis.
The treatment goals are preservation of beta-cell function and strict glycemic control.
C-peptide < 0.3 nmol/L: Choose insulin-based treatment similar to T1D
High C-peptide: In addition to insulin therapy, combination with other glucose-lowering drugs is recommended (International Expert Panel recommendation)
SU drugs are contraindicated: They increase β-cell load, leading to worsening function and poor glycemic control5)
SGLT2 inhibitors: Benefit in LADA is not established
As a protective effect of DPP-4 inhibitors, a report maintains HbA1c at 5.9% for one year in a 90-year-old woman with sitagliptin 100 mg/day3). Also, in a case of LADA with Hashimoto’s disease where HbA1c worsened from 7.9% to 11.7%, metformin, sitagliptin, gliclazide 120 mg/day, dapagliflozin, and dulaglutide were all ineffective, but insulin basal-bolus achieved HbA1c 5.7%5).
Iridocyclitis: Rapid improvement with steroid eye drops.
QWhy can sulfonylureas (SUs) not be used in the treatment of LADA?
A
SUs directly act on beta cells to forcibly promote insulin secretion, increasing the burden on beta cells and further impairing the function of remaining beta cells that are being depleted by autoimmunity. The use of SUs in LADA has been reported to lead to poor glycemic control 5), and their use is contraindicated.
The characteristics of autoantibodies in LADA are shown below.
Antibody
Characteristics
GAD65
Most common in both T1DM and LADA
ICA
High positivity rate in both T1DM and LADA
IA-2A and IAA
High positivity rate in T1DM alone
GAD65 is present not only in pancreatic islets but also in the thyroid, brain, pituitary, kidney, liver, adrenal glands, ovaries, and testes4). Therefore, high titers of GAD65 antibodies are associated with an increased risk of thyroid autoimmunity, and the prevalence of thyroid disease in LADA patients reaches 17.7%5).
The mechanism on the T1DM side is based on the pathway: genetic predisposition → immunological factors → β-cell apoptosis via autoantibodies → insulin deficiency. On the T2DM side, the mechanism involves: obesity → visceral fat accumulation → mild inflammation → autoimmunity → β-cell dysfunction.
Lee et al. (2023) reported a case of a 46-year-old man with a history of T2DM who tested positive for IA2 antibodies (20.6 DK units/mL, normal < 5.4) after COVID-19 infection and was diagnosed with LADA1). ACE2 receptors are expressed in pancreatic exocrine glands and islet cells, and the SARS-CoV-2 spike protein binds to ACE2, is primed by TMPRSS2, and enters cells. A cascade has been proposed: ACE2 inhibition → angiotensin II elevation → sustained NHE2 activation → increased reactive oxygen species → oxidative stress → insulin resistance and β-cell injury.
Chronic hyperglycemia damages retinal blood vessels earliest and most frequently, causing diabetic retinopathy. In neuropathy, metabolic injury leads to atrophy of Aδ and C fibers (small fiber neuropathy), causing pain and burning sensations starting in the feet.
Autoimmune Chain (Association with Sjögren’s Syndrome and Hashimoto’s Thyroiditis)
Wen et al. (2021) reported that two middle-aged women with Sjögren’s syndrome (SS) and Hashimoto’s thyroiditis (HT) maintained normal glucose tolerance on OGTT for 3 years despite being positive for GAD65-Ab or IAA-Ab4). Autoantibody positivity does not immediately mean progression to LADA; onset occurs only when promoting factors such as obesity are added.
7. Latest Research and Future Prospects (Investigational Reports)
Teplizumab is an anti-CD3 monoclonal antibody approved by the FDA in November 2022. It binds to CD3 on T cells and inactivates autoreactive T cells, thereby delaying the onset of T1DM. It is not approved or studied for LADA, but due to the common autoimmune mechanism, it is expected to potentially delay onset.
Semaglutide and Risk of Non-Arteritic Anterior Ischemic Optic Neuropathy
Hathaway et al. (2024) reported that in patients with T2DM, the risk of non-arteritic anterior ischemic optic neuropathy was significantly higher in the semaglutide group, with an HR of 4.28 (95% CI 1.62-11.29, P < 0.001)6). When using GLP-1RAs in LADA, attention should be paid to the development of non-arteritic anterior ischemic optic neuropathy.
Rapid reduction in HbA1c is associated with an increased risk of worsening diabetic retinopathy, including progression of proliferative retinopathy and new-onset macular edema. Ophthalmic monitoring is important when initiating GLP-1RAs, including semaglutide.
Marcon et al. (2022) reported a case of a 90-year-old woman positive for GAD65 > 250 U/ml who was treated with sitagliptin 100 mg/day and maintained HbA1c at 5.9% for one year3). DPP-4 inhibitors may delay beta-cell destruction in LADA, but further RCTs are needed.
Gupta et al. (2023) reported a case of a LADA patient (44-year-old male) diagnosed with DKA who, after CGM initiation, experienced blood glucose fluctuations of 80-408 mg/dL, leading to worsening of pre-existing OCD and suicide 2). DM patients have approximately twice the risk of depression, highlighting the importance of psychiatric evaluation before CGM use.
Large-scale studies on the incidence of pancreatic islet autoantibodies (IA2, GAD65, ICA) in COVID-19 patients are needed 1). Additionally, long-term follow-up studies are required to determine whether non-diabetic patients with GAD65-Ab positivity and SS/HT will progress to LADA in the future 4).
QCan teplizumab be used for LADA?
A
Currently, it is only FDA-approved for T1DM. Since LADA shares a similar autoimmune mechanism, it may theoretically be effective, but research and approval have not been conducted. Future clinical trials are anticipated.
Lee N, Prabhu P, Swaminath S, et al. Development of Islet Antigen 2 (IA2) Antibodies Post-COVID-19 Infection: A Sign of Autoimmunity or Latent Autoimmune Diabetes Mellitus in Adults (LADA)? Cureus. 2023;15(6):e40971. doi:10.7759/cureus.40971.
Gupta R, Edupuganti S, Zamir I, et al. Latent Autoimmune Diabetes in Adults and a Continuous Glucose Monitoring Device: An Unfortunate Outcome. Cureus. 2023;15(11):e49141. doi:10.7759/cureus.49141.
Marcon LMR, Fanelli CG, Calafiore R. Type 1 Diabetes (T1D) and Latent Autoimmune Diabetes in Adults (LADA): The Difference Between a Honeymoon and a Holiday. Case reports in endocrinology. 2022;2022:9363543. doi:10.1155/2022/9363543. PMID:35355800; PMCID:PMC8960035.
Wen S, Jiang W, Zhou L. Islet Autoantibodies in the Patients with Sjogren’s Syndrome and Thyroid Disease and Risk of Progression to Latent Autoimmune Diabetes in Adults: A Case Series. Diabetes Metab Syndr Obes. 2021;14:1025-1033. doi:10.2147/dmso.s295847.
Ibrahim A, Ahmed Mohmed MH, Darwish H, Maximus P, Rezzek M, Daoud MH, et al. A Case of Persistent Hyperglycemia: Autoimmune Link Between Hashimoto’s Thyroiditis and Latent Autoimmune Diabetes in Adults. Cureus. 2025;17(8):e91219. doi:10.7759/cureus.91219. PMID:41024896; PMCID:PMC12476572.
Hathaway JT, Shah MP, Hathaway DB, et al. Risk of Nonarteritic Anterior Ischemic Optic Neuropathy in Patients Prescribed Semaglutide. JAMA Ophthalmol. 2024. doi:10.1001/jamaophthalmol.2024.2296.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.