Chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) is a disease in which the myelin sheaths of peripheral nerves are damaged by immune-mediated mechanisms. The prevalence is 0.8 to 8.9 per 100,000 people, and it can occur at any age, with a slight male predominance. The prevalence in Japan (Tottori Prefecture) is reported to be 0.8 per 100,000 people.
CIDP is primarily a polyneuropathy characterized by limb weakness and sensory disturbances, but it can also affect cranial nerves. Cranial nerve involvement is observed in approximately 15% of cases 1), and among these, ocular symptoms are particularly important as neuro-ophthalmic manifestations.
If ophthalmologists overlook the neuro-ophthalmic complications of CIDP, appropriate systemic treatment may be delayed, potentially leading to irreversible visual impairment. Therefore, accurately understanding the characteristics of ophthalmic complications in CIDP is clinically crucial.
QWhat kind of disease is CIDP?
A
CIDP stands for chronic inflammatory demyelinating polyradiculoneuropathy, a disease in which the myelin sheaths of peripheral nerves are damaged by autoimmune mechanisms. It is characterized by limb weakness, sensory disturbances, and loss of deep tendon reflexes, and is diagnosed when symptoms persist for more than 2 months or recur three or more times. In about 15% of cases, cranial nerves are also affected, presenting neuro-ophthalmic complications such as ophthalmoplegia, papilledema, and optic neuropathy.
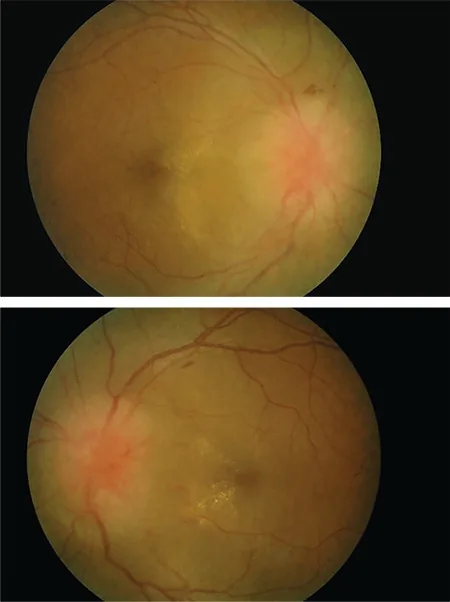
Mas Edi Putriku Intan Ab Kahar, Julieana Muhammed, Wan Hazabbah Wan Hitam et al. Bartonella henselae Neuroretinitis: A Rare Coinfection in POEMS Syndrome. Turkish Journal of Ophthalmology. 2020 Dec 29; 50(6):371. Figure 1. PMCID: PMC7802104. License: CC BY.
The main subjective symptoms reported by patients as neuro-ophthalmic complications of CIDP are as follows.
Diplopia is the most common ophthalmic complaint, caused by impairment of the extraocular muscles or their innervating nerves. Ptosis occurs due to oculomotor nerve (third cranial nerve) dysfunction and may precede or accompany diplopia. Visual acuity loss and visual field defects are observed in optic neuropathy or severe papilledema, and if left untreated, can lead to permanent visual dysfunction. Proptosis may occur due to space-occupying effects from nerve hypertrophy or inflammation within the orbit, although it is rare but reported.
Differential diagnosis: Requires differentiation from optic neuritis, POEMS, and diabetic neuropathy.
Treatment: Immunotherapy (steroids, IVIg) is often effective.
Proptosis and pupillary abnormalities
Proptosis: Due to orbital nerve hypertrophy or inflammatory infiltration. A rare complication.
Pupillary abnormalities: Mydriasis due to oculomotor nerve palsy and pupillary abnormalities due to autonomic dysfunction have been reported.
Autonomic dysfunction: CIDP may be accompanied by autonomic dysfunction, and some cases show Adie pupil-like findings.
Diagnostic significance: Orbital MRI is useful for differentiating proptosis.
QHow common is ophthalmoplegia in CIDP?
A
The frequency of ophthalmoplegia in CIDP is reported to be 3–8% 1). Among cranial nerve involvement (approximately 15%), ophthalmoplegia is a major complication, with the abducens nerve (cranial nerve VI) being particularly susceptible, leading to diplopia. It has been suggested that patients positive for anti-sulfatide IgM antibodies are more likely to develop ophthalmoplegia, and early initiation of immunotherapy may lead to improvement.
The pathogenesis of CIDP is autoimmune demyelination, involving T-cell-mediated and antibody-mediated mechanisms. Autoimmune reactions against myelin-associated proteins (P0, P2, PMP22) form the basis of the pathology.
The diagnosis of CIDP is based on the 2021 EAN/PNS diagnostic criteria, integrating clinical, electrophysiological, laboratory, and neuroimaging findings 4). The 2021 criteria have a sensitivity of 74–83% and specificity of 94–98%, with simplified diagnostic categories compared to the 2010 criteria 4).
After a confirmed diagnosis of CIDP, or if neuro-ophthalmic symptoms appear before confirmation, the following tests are important.
Test
Purpose
Findings
Cerebrospinal fluid examination
Confirmation of protein elevation
Protein elevation (normal cell count is typical); in Bahramy 2024 case, protein 210 mg/dL2)
QWhat role does neuroimaging play in the diagnosis of CIDP?
A
In the 2021 EAN/PNS diagnostic criteria, nerve ultrasound and MRI are specified as ancillary diagnostic criteria for cases that do not meet electrophysiological criteria 4). Marked hypertrophy of peripheral nerves is highly specific for CIDP and CMT1, and its confirmation contributes to improved sensitivity. Orbital MRI evaluates hypertrophy or infiltration of the optic nerve and intraorbital nerves, and is useful for the differential diagnosis of proptosis.
The basic principle of treatment for neuro-ophthalmic complications of CIDP is to control the underlying disease with systemic immunotherapy. Treatment should be carried out in close collaboration between neurologists and ophthalmologists.
First-line treatment includes the following three established options.
Corticosteroids such as oral prednisolone or intravenous methylprednisolone are used to suppress demyelination through anti-inflammatory and immunosuppressive effects. Long-term use requires caution regarding the risk of cataracts, glaucoma, and infections, and regular ophthalmologic check-ups are recommended.
Intravenous immunoglobulin (IVIg) therapy at a standard dose of 2 g/kg (divided over 5 days) is effective for improving neurological symptoms in the acute phase 1). In a case of ocular muscle palsy reported by Chen 2023, complete recovery was achieved within 3 months with a combination of IVIg and glucocorticoids 1).
Plasmapheresis (plasma exchange) is used for cases that do not respond to the above treatments, aiming to remove autoantibodies.
For refractory or recurrent cases, immunosuppressive agents such as rituximab, bortezomib, azathioprine, and cyclosporine are used. In a case of CIDP after COVID-19 vaccination reported by Kim 2023, treatment was performed with a triple combination of prednisolone, azathioprine, and IVIg3).
For refractory papilledema, intracranial pressure-lowering therapy with acetazolamide and optic nerve sheath fenestration may be necessary to preserve visual function.
QIs IVIg effective for ophthalmoplegia in CIDP?
A
IVIg is effective for ophthalmoplegia in CIDP. In a CIDP case with ophthalmoplegia reported by Chen 2023, combination therapy with IVIg (2 g/kg over 5 days) and glucocorticoids resulted in complete improvement of eye movements after 3 months 1). IVIg often suppresses acute inflammation of peripheral nerves and leads to rapid symptom improvement. However, regular maintenance therapy may be required in some cases.
The mechanism of neuro-ophthalmic complications in CIDP is the same as that of peripheral neuropathy. Autoimmune T cells and autoantibodies act on the myelin or axons of oculomotor nerves and optic nerves, causing dysfunction.
Chen L et al. (J Int Med Res. 2023) analyzed 14 patients including those with CIDP presenting with ophthalmoplegia and showed an association between anti-sulfatide IgM antibody positivity and ophthalmoplegia. In that study, hypertrophy of the cervical and brachial plexus was confirmed in 8 of 14 patients (57%), and the group with nerve hypertrophy had a significantly longer disease duration (mean 15.9 years) compared to the group without hypertrophy (3.3 years) 1).
Bahramy MA et al. (BMC Neurol. 2024) reported a case of CIDP after Sinopharm (inactivated) vaccination. Cerebrospinal fluid protein was markedly elevated at 210 mg/dL (normal < 45 mg/dL), and white blood cell count was 4/μL, within normal range2).
Kim S et al. (J Korean Med Sci. 2023) reported two cases of CIDP after mRNA-1273 and Ad26.COV2.S vaccination3). In both cases, symptom onset occurred within a few weeks after vaccination, but a causal relationship has not been established. CIDP after COVID-19 vaccine is thought to involve molecular mimicry, adjuvant effects, and immune activation, but at present, coincidental association cannot be ruled out.
Rathore H, Thaker N (Indian J Nucl Med. 2023) reported a case where a patient followed for CIDP-like symptoms was later found to have POEMS syndrome5). Papilledema is included as a minor diagnostic criterion for POEMS, and evaluation of serum M protein, VEGF, and organomegaly is essential for differentiating CIDP from POEMS.
The 2021 EAN/PNS diagnostic criteria revised the 2010 criteria, with diagnostic accuracy validated as sensitivity 74–83% and specificity 94–98% 4). A major improvement is the formal inclusion of nerve ultrasound and MRI as supportive diagnostic criteria. Marked enlargement of peripheral nerves is highly specific for CIDP and CMT1, contributing to improved diagnostic sensitivity in cases that do not meet electrophysiological criteria 4).
Cases of CIDP onset after COVID-19 vaccination have been reported worldwide, accumulating across viral vector vaccines, mRNA vaccines, and inactivated vaccines 2, 3). However, establishing a causal relationship requires epidemiological comparison of incidence rates and elucidation of biological mechanisms; at present, coincidental association cannot be ruled out.
Anti-nodopathy antibodies and treatment responsiveness
Anti-nodopathy antibodies such as anti-NF155, anti-CNTN1, and anti-CASPR1 antibodies are associated with specific subtypes of CIDP and have been shown to correlate with poor response to IVIg and severe cases. Precision medicine approaches based on these antibody profiles are expected as future treatment strategies. The significance of anti-sulfatide IgM antibodies in cases presenting with ophthalmoplegia also requires further investigation 1).
Chen L, Dong W, Li J, et al. Chronic inflammatory demyelinating polyneuropathy with ophthalmoplegia and anti-sulfatide IgM antibody positivity: a case report and literature review. J Int Med Res. 2023;51(9):3000605231198994.
Bahramy MA, Moridnejad M, Shariati M, et al. Chronic inflammatory demyelinating polyneuropathy following COVID-19 vaccination: a case report. BMC Neurol. 2024;24(1):294.
Kim S, Lee EK, Sohn E. Two Case Reports of Chronic Inflammatory Demyelinating Polyneuropathy After COVID-19 Vaccination. Journal of Korean medical science. 2023;38(8):e57. doi:10.3346/jkms.2023.38.e57. PMID:36852853; PMCID:PMC9970789.
Kuwabara S, Suichi T. Validation of the 2021 EAN/PNS diagnostic criteria for chronic inflammatory demyelinating polyneuropathy. J Neurol Neurosurg Psychiatry. 2022;93(12):1237-1238.
Rathore H, Thaker N. POEMS Syndrome Masquerading as Chronic Inflammatory Demyelinating Polyneuropathy. Indian J Nucl Med. 2023;38(1):59-62.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.