Diabetic papillopathy (DP) is a relatively rare optic disc edema that occurs in patients with diabetes. It was first reported in 1971 by Lubow and Makley in young patients with type 1 diabetes. The incidence is low, about 0.5%, but it can occur at any age in both type 1 and type 2 diabetes.
The essence of DP is considered to be mild, reversible ischemia in the optic nerve head (ONH) region 2). It has also been proposed that DP represents one end of a spectrum of optic disc ischemia, ranging from disc edema without functional impairment to clear infarction in NA-AION 2).
A characteristic of DP is that despite marked disc edema, the impact on visual acuity and visual field is minimal. Relative afferent pupillary defect (RAPD) is mild, and severe visual field defects are usually absent 2). Disc edema resolves spontaneously and rarely leaves optic atrophy2).
Some authors consider DP as a form of NA-AION, but its pathological position remains inconclusive. Diagnosis is one of exclusion, and differentiation from other diseases is necessary (see “Diagnosis and Examination Methods” section).
QIs diabetic papillopathy related to the severity of diabetic retinopathy?
A
There is no clear relationship. DP can occur without diabetic retinopathy (DR). On the other hand, reports indicate that DR coexists in 63-80% of cases, so the two conditions frequently occur together. No correlation has been found between the severity of DR and the development of DP 1).
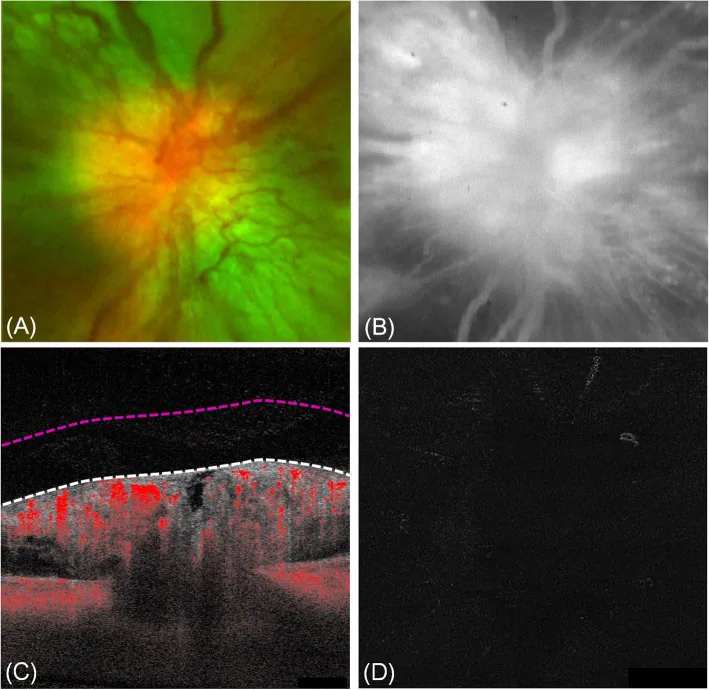
Ji Min Choi; Hye Jin Lee; Dae Joong Ma. Swept-source optical coherence tomography angiography of diabetic papillopathy: a case report. BMC Ophthalmol. 2020 May 15; 20:194. Figure 2. PMCID: PMC7229636. License: CC BY.
Diabetic papillopathy. a Fundus photography revealed a swollen optic disc, splinter hemorrhages, and dilated vessels over the optic disc. b Fluorescein angiography showed an early hyperfluorescence by fluorescein leaks from the disc vessels. c The B-scan image displayed blood flow signals in the thickened retinal nerve fiber layer of the optic disc and no flow signal above the vitreoretinal interface (VRI, white dashed line). d The correlating VRI slab (between white and red dashed line in c) image did not depict signal flow
Many patients are asymptomatic and are discovered incidentally during regular diabetic eye examinations. Even when symptoms are present, they are mild.
Asymptomatic: Most patients lack subjective symptoms.
Blurred vision: Some patients may complain of this.
Decreased vision (mild): Often improves without significant vision loss.
A characteristic feature of DP is the discrepancy between the degree of optic disc edema and its impact on visual acuity and visual field. The main clinical findings of DP are shown below.
Dilated microvessels on the optic disc surface are observed in about 50% of cases. Importantly, this vascular dilation does not extend into the vitreous, distinguishing it from neovascularization of the disc (NVD) in proliferative diabetic retinopathy.
Macular edema (ME) is present in over 50% of cases 1). Additionally, a crowded optic disc in the fellow eye is frequently reported 2). Papilledema often resolves spontaneously after up to 12 months, leaving little optic atrophy2).
In case 1 reported by Arapi et al. (2021) (60-year-old female, type 2 DM, HbA1c 10.9%), the right eye showed visual acuity of 6/360 and severe papilledema with splinter hemorrhage. Seven weeks after treatment, visual acuity recovered to 20/30 1).
The pathogenesis of DP is not fully understood, but diabetic microangiopathy is considered to be the underlying cause. It occurs in both type 1 and type 2 diabetes.
The main risk factors are as follows:
Poor glycemic control: Frequently reported in cases with high HbA1c (e.g., HbA1c 10.9%, 11.2%) 1).
Rapid glycemic control: Rapid improvement in blood glucose, such as with new insulin initiation, is thought to contribute to onset.
Crowded optic disc: Dense packing of nerve fibers within the disc increases the risk of vascular compression 2).
Optic disc drusen: Abnormal deposits within the optic disc have been identified as a risk factor.
DM is listed as a risk factor for NA-AION, and DP and NA-AION may share a common pathological basis2).
QDoes rapidly lowering blood glucose increase the risk of developing it?
A
Rapid glycemic control (e.g., initiation of insulin therapy) is thought to contribute to the development of DP. It is hypothesized that a sharp drop in blood glucose leads to fluid accumulation around the optic disc, causing disc edema. Ophthalmologic follow-up is important when starting insulin therapy.
Fluorescein angiography (FA/FFA): In DP, very early leakage (fluorescein leakage from dilated superficial optic disc vessels) is characteristic 2). The absence of filling delay helps differentiate it from NA-AION 1). In optic discneovascularization, random leakage into the vitreous is seen, whereas in DP there is no extension into the vitreous.
Optical coherence tomography (OCT): Useful for confirming increased retinal nerve fiber layer (RNFL) thickness and macular edema (ME) 1).
QHow is it different from NA-AION (non-arteritic anterior ischemic optic neuropathy)?
A
DP is characterized by negative RAPD, minimal visual field defects, and spontaneous improvement. NA-AION presents with altitudinal hemianopia, clear RAPD, and optic atrophy. On FA, DP shows very early leakage from the optic disc surface, while NA-AION shows delayed filling 2). Both are considered to be a continuous spectrum of ONH ischemia 2).
Observation is the mainstay. DP often resolves spontaneously within 3 to 6 months (up to 12 months), with disc edema subsiding while maintaining vision.
Observation
First choice: Many cases show spontaneous resolution of disc edema with 3 to 6 months of observation.
Blood glucose control: Maintain stable control avoiding rapid glucose fluctuations.
Steroid Therapy
Sub-Tenon injection (STTAI): Uses triamcinolone 40 mg/mL. Lower risk of intraocular pressure elevation than IVTA. Subtenon betamethasone has been reported to shorten the natural course from 5 months to 3 weeks 1). IVTA (intravitreal injection) has about 3 times higher risk of IOP elevation (>21 mmHg) compared to STTAI.
Anti-VEGF + Steroid Combination
IAI (aflibercept 2 mg/0.05 mL) + STTAI (TA 40 mg/mL): Combination therapy reported for severe cases 1).
Effect: Papilledema and visual acuity recover within 5–7 weeks. Stability is maintained during 12 months of follow-up 1).
Other: There are also reports of anti-VEGF monotherapy with ranibizumab or bevacizumab.
Arapi et al. (2021) performed combination therapy with IAI (aflibercept 2 mg) and STTAI (triamcinolone 40 mg/mL) in two cases of severe DP 1). Case 1 (HbA1c 10.9%) improved from 6/360 in the right eye to 20/30 after 7 weeks, and from 6/60 in the left eye to 20/25 after 5 weeks. Case 2 (HbA1c 11.2%) recovered from 6/120 in the left eye to 20/30 after 5 weeks. Both showed a stable course during 12 months of follow-up.
QWill it resolve on its own without treatment?
A
Many cases resolve spontaneously within 3–6 months (up to 12 months), and 92% maintain visual acuity. Observation is the first choice. In severe cases or those with significant macular edema, treatment with steroids or anti-VEGF may promote recovery 1).
The pathology of DP is based on diabetic microangiopathy. The main proposed mechanisms are as follows.
Epi/peripapillary microangiopathy: Capillary damage around the optic disc increases vascular permeability, leading to papilledema1).
Deep laminar circulation disorder and disruption of axonal flow: Blood flow impairment at the level of the lamina cribrosa interferes with axonal transport, causing swelling of the optic nerve fibers 1).
Water accumulation due to rapid glycemic control: A rapid decrease in blood glucose alters tissue osmotic pressure, leading to fluid accumulation around the optic disc. This is thought to compress the lamina cribrosa and reduce axonal flow.
Mild, reversible ischemia of the prelaminar ONH: DP is considered a mild end of the spectrum of ONH ischemia 2). Some view it as a continuous condition that can progress to NA-AION if it becomes severe 2).
Interaction between inflammatory cytokines and VEGF: Overproduction of VEGF in diabetic microangiopathy contributes to increased vascular permeability 1).
7. Latest Research and Future Perspectives (Investigational Reports)
Combination therapy of anti-VEGF agents (aflibercept, ranibizumab, bevacizumab) and steroids for DP has been reported to be effective in severe cases at the case report level. Arapi et al. showed that combination therapy promotes visual recovery and resolution of optic disc edema in severe DP 1). However, currently limited to case reports, standardization of treatment protocols requires large-scale prospective studies 1).
Salvetat et al. (2023) positioned DP as the mild end of the ONH ischemic spectrum and discussed the possibility that DP and NA-AION form a pathologically continuous disease group 2). This perspective is important for identifying prognostic factors and determining the timing of therapeutic intervention in DP. Development of biomarkers and imaging diagnostic indicators that define the boundary between the two is a future challenge 2).
Arapi I, Neri P, Giovannini A, Grezda A. Combined therapy with intravitreal aflibercept and subtenon corticosteroids in eyes with severe diabetic papillopathy: two case reports. J Med Case Reports. 2021;15:518. doi:10.1186/s13256-021-03129-1. PMID:34674724; PMCID:PMC8532332.