Iridocorneal endothelial (ICE) syndrome is a disease in which abnormal corneal endothelial cells extend and contract into the angle and iris with a membranous tissue, obstructing the trabecular meshwork and causing elevated intraocular pressure. It is characterized by corneal edema due to corneal endothelial abnormality, iris deformation due to contraction of the membranous tissue, and peripheral anterior synechiae (PAS).
ICE syndrome is classified into the following three clinical types.
Chandler syndrome: Most common (about 50%). Corneal edema is predominant, with mild iris findings.
Progressive iris atrophy: Iris hole formation, pupillary deviation, and uveal ectropion are prominent. Most frequently associated with glaucoma.
Cogan-Reese syndrome: Characterized by pigmented nodules on the iris surface. The rarest subtype 4).
It usually occurs unilaterally in women aged 20–50 years 2). It is sporadic and has no consistent association with other ocular or systemic diseases. ICE syndrome is unilateral and sporadic, which is the simplest distinguishing point from bilateral, hereditary posterior polymorphous corneal dystrophy (PPMD).
QHow are the three types of ICE syndrome differentiated?
A
The differentiation of the three types is mainly based on clinical findings of the iris and cornea. Chandler syndrome is characterized by corneal edema with minimal iris changes, and corneal edema can occur even with normal intraocular pressure. Progressive iris atrophy features polycoria, pupillary deviation, iris hole formation, and uveal ectropion, and is most frequently associated with glaucoma. Cogan-Reese syndrome is characterized by pedunculated brown nodules or diffuse pigmented lesions on the iris surface, and iris atrophy is usually absent. However, all types share a common pathophysiology and similar treatment approach.
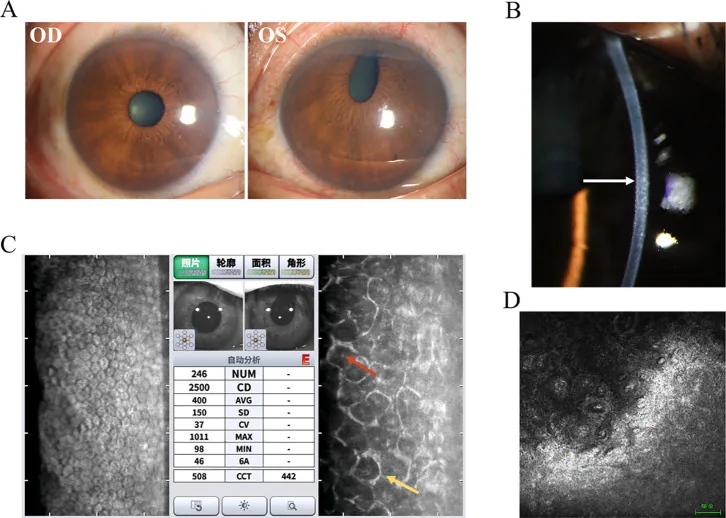
Clinical and ancillary test findings of Chandler syndrome: (A) iris loss and pupillary distortion, (B) hammered silver appearance of corneal endothelium, (C) ICE cells on specular microscopy, (D) epithelioid endothelial cells on confocal microscopy. Corresponds to corneal endothelial abnormalities discussed in section “2. Main Symptoms and Clinical Findings”.
Initial symptoms include unilateral pain, blurred vision, or changes in iris appearance. Pain due to corneal edema and pain from elevated intraocular pressure due to angle closure may coexist. Some patients present after noticing iris heterochromia or pupillary distortion.
Corneal findings: The corneal endothelium has a “beaten silver” or “hammered copper” appearance, resembling the guttae of Fuchs endothelial corneal dystrophy. Corneal edema may be microcystic even with normal intraocular pressure.
Iris findings: Iris heterochromia, uveal ectropion, pupillary deviation, iris hole formation, and iris atrophy appear depending on the subtype 2). In Cogan-Reese syndrome, pigmented nodules on the iris surface are observed, which histologically are benign lesions composed of melanin-containing spindle-shaped nevus cells 4).
Angle findings: Gonioscopy reveals peripheral anterior synechiae extending high beyond the Schwalbe line, which is pathognomonic for ICE syndrome5). The peripheral anterior synechiae are patchy and located very anteriorly, and the trabecular meshwork between the synechiae appears normal 5).
The true etiology of ICE syndrome remains unknown, but there is a hypothesis that latent infection with herpes simplex virus (HSV) or Epstein-Barr virus (EBV) induces low-grade inflammation at the corneal endothelial level, leading to epithelial-like activation. PCR testing has detected HSV DNA at high rates in the corneal endothelium and aqueous humor of patients with ICE syndrome, with multiple reports detecting HSV DNA in over 60% of patient corneal and aqueous humor samples 2).
Pathologically, normal endothelial cells are replaced by epithelial-like cells with migratory properties. Electron microscopy reveals epithelial features such as desmosomes, tonofilaments, and microvilli. Toxic damage (necrotic changes) to adjacent normal endothelial cells has also been reported.
Specular microscopy: The most important diagnostic tool 2). The typical hexagonal corneal endothelial shape is lost, showing pleomorphism and “light-dark reversal.” Characteristically, larger and darker endothelial cells (ICE cells) with a bright central spot are seen. A marked decrease in corneal endothelial cell density is observed, with one case of Cogan-Reese syndrome reported to have decreased to 763 cells/mm² 3).
In vivo confocal microscopy (IVCM): Depicts cobblestone-like swollen cells of the corneal endothelium, loss of hexagonal structure, pleomorphic hyperreflective cells, and mononuclear and binuclear giant endothelial cells 2).
Anterior segment OCT (AS-OCT): Visualizes iridocorneal angle adhesions, hyperreflective thickening of the corneal endothelial layer, and membranous tissue on the iris2).
Gonioscopy: Essential for evaluating peripheral anterior synechiae, used for diagnosis and follow-up of secondary angle-closure glaucoma.
Glaucoma evaluation: Intraocular pressure measurement, optic disc photography, visual field testing (Humphrey or Goldmann), and OCT evaluation of the retinal nerve fiber layer should be included in initial workup and follow-up 2).
QWhy is ICE syndrome sometimes misdiagnosed as open-angle glaucoma?
A
The advancing corneal endothelial cell membrane may functionally close the trabecular meshwork without contraction. In such cases, gonioscopy may not reveal obvious peripheral anterior synechiae, leading to misdiagnosis as open-angle glaucoma despite the presence of “functional” angle closure. When encountering unilateral glaucoma, ICE syndrome should be considered in the differential diagnosis, and the corneal endothelium should be carefully evaluated with specular microscopy.
Aqueous humor production suppressants: Topical beta-blockers, alpha-agonists, and carbonic anhydrase inhibitors are first-line treatments 6). Aqueous humor production suppressants are recommended over miotics that target the aqueous humor outflow pathway.
Prostaglandin-related drugs: Due to the theoretical role of HSV, there is concern about latanoprost-induced HSV recurrence, and careful consideration is warranted 2).
Corneal edema management: Corneal dehydration is performed using hypertonic saline eye drops or gel.
Long-term prognosis: Drug treatment often becomes resistant as the membranous tissue progresses and peripheral anterior synechiae expand 6).
Surgical Treatment
Trabeculectomy: Performed with adjunctive antifibrotic agents (MMC or 5-FU) 6). Reported survival rates are 73% at 1 year, 44% at 3 years, and 29% at 5 years. There is a risk of fistula occlusion by abnormal endothelium.
Tube shunt surgery: Survival rates are 71% at 1 year, 71% at 3 years, and 53% at 5 years, showing better long-term outcomes than trabeculectomy5)6). Tube shunts with a plate are often chosen.
Corneal endothelial transplantation: DSAEK/DSEK improves corneal function 1). Graft survival is comparable to penetrating keratoplasty (PKP), but visual recovery is faster and astigmatism is milder 1).
Cyclodestructive procedures: Diode laser cyclophotocoagulation is performed as a last resort for refractory cases 6).
A two-stage surgical approach has been reported: phacoemulsification with artificial iris implantation is performed first, followed by DSAEK 6 months later 1). In a case of a 54-year-old woman, postoperative corrected visual acuity improved from 20/100 to 20/32, and corneal endothelial cell density of 1,640 cells/mm² was maintained 1).
A rare complication of cystoid macular edema (CME) in Cogan-Reese syndrome has been reported 3). It resolved with topical NSAIDs (flurbiprofen 3 times daily) but recurred after discontinuation 3). It is hypothesized that abnormal endothelial cells disrupt the inner blood-retinal barrier, and prostaglandin production via HSV-related cytokines is involved in the pathogenesis 3).
The fundamental abnormality in ICE syndrome is epithelialization of the corneal endothelium. Normal endothelial cells are replaced by epithelial-like cells with proliferative and migratory capacity. This process is also common to PPMD, but ICE is unilateral and sporadic, whereas PPMD is bilateral and autosomal dominant.
Epithelialized endothelial cells advance from the posterior corneal surface across Schwalbe’s line onto the trabecular meshwork and further onto the anterior iris surface 5). Contraction of this membrane-like tissue leads to the following conditions.
Secondary angle-closure glaucoma: The main mechanism is obstruction of aqueous outflow due to formation of extensive peripheral anterior synechiae5). Functional closure of the trabecular meshwork by the membrane itself can also occur, so glaucoma may develop even without obvious peripheral anterior synechiae.
Corneal edema: Caused by both pump dysfunction of degenerated endothelial cells and elevated intraocular pressure due to glaucoma. It is most prominent in Chandler syndrome.
Iris deformation: Contraction of the membrane-like tissue pulls the iris, resulting in corectopia, iris hole formation, and ectropion uveae. It is most prominent in progressive iris atrophy, and corectopia is directed toward the area with more peripheral anterior synechiae.
Iris nodules in Cogan-Reese syndrome are histologically composed of spindle-shaped melanocytic nevus-like cells, with Ki-67 positivity less than 1% and melan-A positivity, indicating benign lesions 4). Rarely, they are associated with zonular fragility, and diffuse zonular dialysis may be observed during cataract surgery 4).
QHow to differentiate ICE syndrome from posterior polymorphous corneal dystrophy (PPMD)?
A
The simplest distinguishing point is that ICE syndrome is sporadic and unilateral, whereas PPMD is autosomal dominant and bilateral. Specular microscopy also differs: ICE syndrome shows dark areas with central highlights (ICE cells), while PPMD exhibits typical vesicles or band-like structures. PPMD can also involve corectopia and corneal edema, but it is congenital with no gender difference, so the clinical course differs.
Bouvarel H, Hamard P, Agard E, Billant J, El Chehab H, Dot C. Macular edema in Cogan-Reese syndrome. American journal of ophthalmology case reports. 2022;25:101318. doi:10.1016/j.ajoc.2022.101318. PMID:35128161; PMCID:PMC8810354.
Chhadva P, Del Valle Estopinal M, Farid M. Iris Nevus (Cogan-Reese) Syndrome Presenting with Zonular Dehiscence during Cataract Extraction. Case reports in ophthalmology. 2022;13(2):435-440. doi:10.1159/000524823. PMID:35950024; PMCID:PMC9247537.
Pazos M, Traverso CE, Viswanathan A; European Glaucoma Society. European Glaucoma Society - Terminology and guidelines for glaucoma, 6th Edition. Br J Ophthalmol. 2025;109(Suppl 1):1-212. doi:10.1136/bjophthalmol-2025-egsguidelines. PMID:41026937.