Methamphetamine-induced keratitis (MIK) is an inflammatory corneal disease resulting from methamphetamine abuse. It was first reported by Poulsen et al. in 1996.
Methamphetamine is a potent central nervous system stimulant used via oral ingestion, intravenous injection, smoking, and inhalation. Direct pharmacological effects on the cornea, chemical toxicity of contaminants, and behavioral factors combine to cause corneal damage.
MIK exhibits more pronounced neurotrophic features compared to typical infectious keratitis. Corneal ulcers are often progressive, characterized by large infiltrates, stromal necrosis, and severe thinning. Infectious keratitis frequently complicates, and despite aggressive treatment with enhanced antibiotics, rapid corneal melting or perforation may occur 1).
QHow is methamphetamine-induced keratitis different from typical infectious keratitis?
A
MIK has stronger neurotrophic features compared to typical infectious keratitis. Because corneal sensation is lost, subjective symptoms are mild, leading to delayed consultation. Also, corneal melting progresses rapidly and is often treatment-resistant 1). Infectious keratitis is often concurrent, and findings of both conditions overlap.
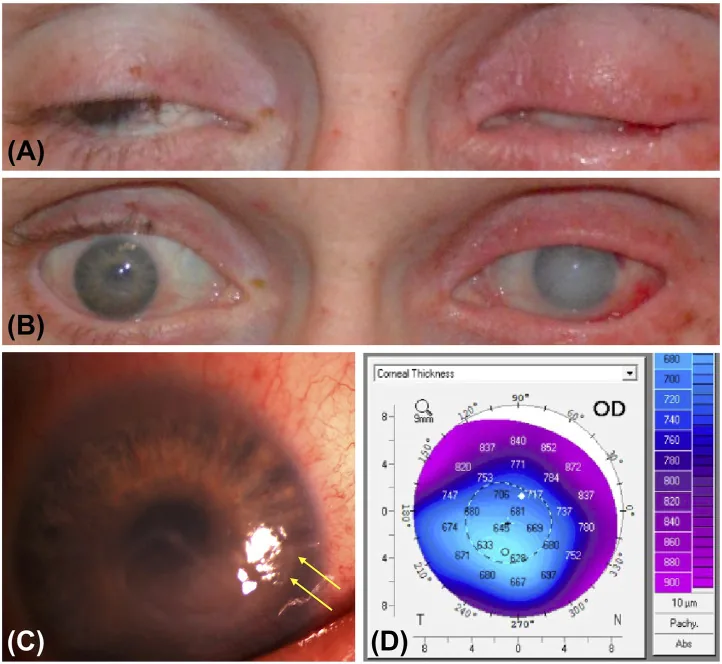
Ye Huang, Nam V Nguyen, Danny A Mammo, Thomas A Albini, et al. Vision health perspectives on Breaking Bad: Ophthalmic sequelae of methamphetamine use disorder 2023 Mar 8 Front Toxicol. 2023 Mar 8; 5:1135792 Figure 1. PMCID: PMC10031494. License: CC BY.
A and B show the appearance with eyes closed and open, with marked eyelid thickening, redness, and conjunctival injection. C shows a slit-lamp image of the right eye with inferior epithelial defect and opacity, and D shows corneal thinning in the same area on Pentacam.
The main complaint is often decreased vision. Patients may present with foreign body sensation, redness, tearing, and photophobia. However, because corneal sensation is reduced, eye pain may be mild.
Descemetocele: A pre-perforation state requiring urgent intervention.
Corneal perforation: Indication for tissue adhesive or therapeutic corneal transplantation.
Endophthalmitis: Occurs when infection spreads into the eye 1).
Huang et al. (2022) reported two cases with methamphetamine use disorder 1). Case 1 was a 26-year-old male with type 1 diabetes and chronic methamphetamine use, presenting with a corneal ulcer caused by Staphylococcus aureus and Streptococcus viridans. Due to poor treatment adherence and persistent eye rubbing, final visual acuity decreased to hand motion in the right eye and light perception in the left eye. Case 2 was a 44-year-old female with dry eye associated with GVHD and a history of methamphetamine use, presenting with diffuse corneal infiltration and hypopyon. Emergency corneal transplantation and vitrectomy were performed, but infection with Streptococcus pyogenes progressed, ultimately leading to enucleation1).
The pathology of MIK involves multiple mechanisms.
Direct pharmacological effects: Vasoconstriction due to the sympathomimetic action of methamphetamine reduces ocular blood flow. Increased pain threshold suppresses the blink reflex, increasing the risk of corneal epithelial damage. Dysregulation of dopamine and serotonin causes corneal neuropathy.
Toxicity of contaminants: Illicit products contain diluents such as lidocaine, procaine, quinine, bicarbonate, and strychnine. These cause corneal alkali injury or ulcers.
Route-related factors: Smoking causes chemical and thermal burns. Direct exposure to methamphetamine hydrochloride smoke damages the cornea. Hand-to-eye contact also worsens corneal damage 1).
Behavioral factors: Hyperactivity and compulsive behavior due to methamphetamine lead to repeated eye rubbing 1). Cognitive decline worsens ocular hygiene.
Comorbidities: Coexisting systemic diseases such as diabetes and GVHD-related dry eye exacerbate corneal damage 1).
QWhich method of methamphetamine use most easily causes corneal damage?
A
Smoking (smoking crystal methamphetamine called “ice”) has been reported to pose the highest risk of corneal ulcers. Methamphetamine hydrochloride in the smoke directly contacts the cornea, causing chemical and thermal burns. However, corneal damage can also occur with other routes such as intravenous injection or inhalation.
A detailed history of drug use (frequency, route of administration, time of last use) is the most important element. Also check contact lens use history, past history of keratitis, and presence of systemic diseases.
Corneal sensitivity test: Using a Cochet-Bonnet esthesiometer. Loss of corneal sensitivity suggests the presence of neurotrophic keratopathy.
Slit-lamp examination: Evaluate the location, shape, and size of corneal infiltrates, extent of epithelial defects, and degree of anterior chamber inflammation. Use fluorescein staining to confirm epithelial damage.
If infectious keratitis is suspected, collect corneal scrapings. Perform smear microscopy (Giemsa stain, Gram stain) and culture to evaluate for bacteria, fungi, HSV/varicella-zoster virus, and Acanthamoeba. Adjust antimicrobial therapy based on culture results.
The choice of antimicrobial agent is based on the severity of corneal damage.
Severity
Antimicrobial Agent
Frequency
Severe
Fortified vancomycin + fortified tobramycin
Every hour
Moderate
Fluoroquinolone such as moxifloxacin
Every hour
Mild
Fluoroquinolone
Every 2–4 hours
Adjust antimicrobials based on culture and sensitivity results. After infection control, if atypical pathogens are ruled out, consider cautious use of steroid eye drops.
QWhat is the prognosis of methamphetamine-induced keratitis?
A
The prognosis is guarded, depending on the severity of keratitis and the presence of behavioral and psychological comorbidities. Poor treatment adherence and continued drug use worsen outcomes1). In severe cases, visual impairment due to corneal scarring may persist, and cases requiring enucleation due to endophthalmitis have been reported1).
The pathology of MIK is multifactorial, with the following mechanisms interrelated.
Vasoconstriction and ocular blood flow impairment: Methamphetamine promotes the release of catecholamines and has strong sympathomimetic effects. Reduced ocular blood flow due to vasoconstriction causes ischemia of corneal tissue 1). Ischemia of the limbal stem cell region may present as diffuse corneal opacity 1).
Neurotrophic keratopathy: Dysregulation of dopamine and serotonin due to methamphetamine use damages corneal nerves. Loss of corneal sensation reduces the blink reflex, leading to tear film instability, impaired epithelial turnover, and delayed corneal wound healing 1). Decreased corneal sensation increases susceptibility to infection, leading to infectious keratitis.
Corneal epithelial barrier disruption: Suppression of the blink reflex due to elevated pain threshold, direct contact with diluents or manufacturing byproducts, and repeated mechanical eye rubbing damage the corneal epithelium. Disruption of the epithelial barrier facilitates microbial invasion and becomes a breeding ground for secondary infection.
Overlapping infection: In many cases, bacterial infection, including gram-positive cocci, is superimposed 1). Poor hygiene, impaired immune function, and corneal fragility increase infection risk. Because infectious keratitis and MIK-specific corneal damage overlap, it may be difficult to determine which is the cause of corneal injury.
Evidence on MIK is mainly based on case reports and small case series; large-scale clinical trials do not exist.
Huang et al. (2022) reported two cases of keratitis and endophthalmitis as ocular complications associated with methamphetamine use disorder, emphasizing a serious association between methamphetamine use and acute corneal findings based on temporal correlation and pharmacological mechanisms 1).
Further elucidation of the pathophysiology of MIK and development of prevention and treatment strategies are future challenges. Community-level education and awareness activities and harm reduction strategies (hand hygiene guidance, avoidance of eye rubbing) have been proposed as preventive interventions. Establishment of a multidisciplinary collaboration model between addiction treatment and ophthalmology is also needed.
Huang Y, Chundury RV, Timperley BD, Terp PA, Krueger RR, Yeh S. Ophthalmic complications associated with methamphetamine use disorder. American journal of ophthalmology case reports. 2022;26:101464. doi:10.1016/j.ajoc.2022.101464. PMID:35282603; PMCID:PMC8907677.
Franco J, Bennett A, Patel P, Waldrop W, McCulley J. Methamphetamine-Induced Keratitis Case Series. Cornea. 2022;41(3):367-369. PMID: 34050072.