Descemet membrane detachment (DMD) is a condition in which the Descemet membrane detaches from the posterior surface of the corneal stroma. It occurs mainly as a complication of intraocular surgery, but can also result from ocular trauma or, rarely, spontaneously. The ICD-10 code is H18.33.
Cataract surgery is the most common setting, with reported incidence rates of 2.5% after extracapsular cataract extraction (ECCE) and 0.5% after PEA. Advances in PEA techniques have reduced the frequency of clinically significant extensive DMD to 0.044%. However, detailed OCT observation reveals micro-DMD in 37.1% of cases on postoperative day 1, decreasing to 4.5% at 1–3 months and disappearing after 3 months.
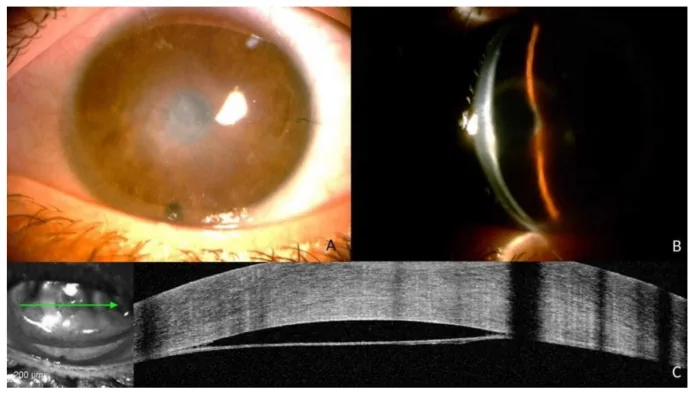
Antonio Moramarco, Danilo Iannetta, Luca Cimino, Vito Romano, et al. Case Report: “Spontaneous Descemet Membrane Detachment” 2022 Dec 31 J Clin Med. 2022 Dec 31; 12(1):330 Figure 1. PMCID: PMC9820967. License: CC BY.
A: Anterior segment photograph with central opacity; B: Slit-lamp view from the side; C: AS-OCT shows extensive Descemet membrane detachment arching away from the posterior corneal surface. The clinical image and tomographic image allow comparison of the detachment extent.
The main complaints are poor visual improvement or sudden vision loss after cataract surgery. Patients may report blurred vision due to corneal edema or foreign body sensation from corneal epithelial irregularity.
Mechanism in cataract surgery: Caused by creating an incision with a dull blade, careless insertion/removal of instruments through a small incision, or inadvertent injection of irrigating solution into the corneal stroma during OVD or hydration. Performing hydration near the inner tunnel flap (near Descemet’s membrane) increases the risk of DMD.
Cataract surgery after DALK: After DALK, there is a cleavage plane between the donor stroma and the host’s pre-Descemet layer. During wound hydration, BSS can reach this cleavage plane and cause DMD due to hydraulic pressure7).
Canaloplasty: Viscoelastic material injected during microcatheter traction accumulates in the inferior quadrant of Schlemm’s canal, exerting pressure beyond the termination of Descemet’s membrane at Schwalbe’s line, leading to DMD. The incidence is higher in combined surgery (phacocanaloplasty)2).
After Nd:YAG laser iridotomy: The shock wave from photodisruption can cause linear tears at the level of Descemet’s membrane, leading to DMD. Shallow anterior chamber and pseudoexfoliation are risk factors8).
Patient factors: Age ≥65 years, Fuchs endothelial corneal dystrophy, cornea guttata, pseudoexfoliation syndrome, corneal dystrophy, diabetes
Intraoperative factors: Dull blade, small incision, inappropriate OVD/irrigating solution injection, anterior chamber entry in shallow anterior chamber, prolonged surgery time
Postoperative factors: Genetic factors involved in poor adhesion between Descemet’s membrane and posterior corneal stroma
QWhy is DMD more likely to occur during cataract surgery after DALK?
A
In DALK, the donor corneal stroma replaces the host’s pre-Descemet layer. This surgery creates a cleavage plane between the donor stroma and the host’s pre-Descemet layer. During cataract surgery, if irrigation fluid reaches this plane during hydration, DMD can easily occur due to hydraulic pressure 7). This DMD is localized within the DALK graft and does not extend to the peripheral host cornea7).
Diagnosis is based on medical history and slit-lamp microscopy, but when corneal edema is prominent, imaging is essential.
Slit-lamp microscopy: If the cornea is clear, the DMD line can be directly observed. In extensive DMD, corneal edema makes detection difficult.
Anterior segment OCT (AS-OCT): A non-contact examination method that accurately identifies the location, shape, extent, and height of DMD. It is the gold standard for diagnosis 4)5). High-resolution swept-source OCT is useful for determining treatment strategy and evaluating treatment efficacy 4).
Gonioscopy: Useful for evaluating localized peripheral DMD.
The HELP algorithm has been proposed as a structured approach to DMD management based on AS-OCT5). It evaluates Height, Extent, Length, and Pupil involvement to determine treatment strategy.
Indications for conservative treatment: Height <100 μm and length <1 mm / height 100–300 μm and 1–2 mm without pupillary involvement.
Indications for surgical treatment: Involvement of the central cornea (within 5 mm) or extensive cases.
Differentiation from corneal stromal edema is important. Stromal edema has an indistinct and irregular border with healthy cornea, whereas DMD has a sharp and arcuate border.
QWhy is AS-OCT important in diagnosing DMD?
A
In extensive DMD, corneal edema makes evaluation with slit-lamp microscopy difficult. AS-OCT provides rapid, non-contact cross-sectional images of the cornea, allowing accurate assessment of DMD location, height, and extent 4). It is also essential for determining treatment strategy based on the HELP algorithm 5) and for confirming reattachment after treatment.
Localized DMD within 1 mm can be managed with observation. Conservative treatment uses topical steroid eye drops (to suppress inflammation and prevent fibrosis) and hypertonic eye drops (to dehydrate the stroma). The spontaneous reattachment rate is reported to be approximately 60%.
This is the gold standard for persistent DMD. Gas is injected into the anterior chamber to reattach the detached Descemet’s membrane to the posterior surface of the corneal stroma. The reattachment success rate is 90–100%, but 4–7% of cases require reinjection.
Gases used:
Air: Used as the first choice. The surgery is completed with total air fill of the anterior chamber, and postoperatively the patient maintains a position where the gas contacts the DMD site.
SF₆ (sulfur hexafluoride): 20% isoexpansile concentration. Retention time approximately 2 weeks. Used for recurrent cases or when initial air injection fails.
C₃F₈ (perfluoropropane): 14% isoexpansile concentration. Retention time approximately 6 weeks. Since SF₆ and C₃F₈ expand, iridotomy or mydriatic treatment is necessary to prevent pupillary block.
Procedure: Gas is injected with a 27–30G needle. After filling the anterior chamber with gas for 15–20 minutes, one-third of the bubble is expelled to prevent pupillary block. Postoperatively, the patient maintains a supine position.
This is a new technique for rolled DMD 1). First, a small bubble is used to unroll the DM, then a larger bubble reattaches the DM. In a 62-year-old woman with extensive DMD after cataract surgery (with rolling), this technique achieved BCVA 6/9 at 6 weeks 1).
After descemetopexy, a partial corneal incision is made with a 23G needle at the deepest part of the DMD to drain residual fluid in the pre-Descemet space 5). In a study of 5 cases, earlier visual recovery (within 1 week) was achieved compared to conventional methods 5). One case required corneal transplantation due to recurrent DMD 5).
In a case of late-onset DMD 45 years after full-thickness corneal transplantation where air/SF₆ descemetopexy was ineffective, partial descemetorhexis of the DM on the central side of the graft-host junction was performed, releasing traction and achieving complete reattachment of the DM 6). This is a new treatment option for tractional DMD without Descemet membrane rupture 6).
Corneal transplantation is considered in cases of recurrent detachment despite multiple gas injections or when bullous keratopathy develops. Approximately 7–8% of all cases require corneal transplantation. DMEK or DSAEK is selected.
Complications of Descemetopexy
Persistent DMD: Most common complication
Elevated intraocular pressure: Especially common with C₃F₈ use
Pupillary blockglaucoma: Reported in up to 13% of cases. Prevented by inferior iridotomy
Uveitis: Rare
Management of Recurrence
Reopacification after corneal clearing: Strongly suspect DMD recurrence and promptly perform gas reinjection
Multiple recurrences: Consider switching from air to SF₆ or C₃F₈
Refractory cases: Consider Descemet membrane suturing or partial descemetorhexis 6)
QShould air or SF₆/C₃F₈ be chosen for intracameral injection?
A
The basic principle is to choose air for the first treatment. Air is safe and causes less damage to the corneal endothelium. In cases of recurrence, SF₆ or C₃F₈ should be considered. These gases have a longer retention time and are effective, but due to their expansile nature, there is a risk of pupillary block and secondary glaucoma. Some opinions suggest that repeating air is safer, considering the corneal endothelial damage caused by long-term gas retention even in recurrent cases.
The mechanism of DMD is the entry of aqueous humor into the pre-descemetic space through a dehiscence in Descemet’s membrane. During corneal incision, a gap is formed between the stroma and Descemet’s membrane, through which irrigation fluid or OVD enters.
Descemet’s membrane is the basement membrane of the corneal endothelium, composed of the anterior banded layer (ABL, about 3 μm thick, formed before birth) and the posterior non-banded layer (PNBL, secreted by endothelial cells throughout life, about 3 μm at age 20, about 10 μm at age 80).
In the cornea after DALK, a cleavage plane exists between the donor stroma and the host pre-Descemet’s layer 7). During cataract surgery, if BSS reaches this plane during hydration, DMD occurs due to hydraulic pressure. Characteristically, DMD is confined to the graft and does not extend to the peripheral host cornea7).
In late-onset DMD after PK, long-term remodeling of scar tissue at the graft-host interface and progression of keratoconus on the host side may cause unbalanced traction on both sides of the interface, leading to DMD 6). This tractional mechanism does not involve Descemet’s membrane dehiscence, and recurrence occurs after air/gas descemetopexy 6).
Shock waves and acoustic pressure waves from photodisruption cause linear cracks at the level of Descemet’s membrane 8). In shallow anterior chambers, the proximity of the cornea to the plasma results in excessive energy transfer to the corneal endothelium. In pseudoexfoliation, diffuse and irregular thickening of Descemet’s membrane and accumulation of pseudoexfoliative material increase vulnerability to DMD 8).
During DSAEK, when inserting the lenticule with a Sheets glide, an irregular glide edge may catch Descemet’s membrane and cause DMD 3). Although an extremely rare complication, early detection and prompt descemetopexy are important to prevent primary graft failure 3).
Köppe MK et al. (2024) used high-resolution swept-source OCT (Anterion) to diagnose DMD and assess treatment efficacy, confirming immediate success of air tamponade for DMD after cataract surgery in a 71-year-old man. They demonstrated that high-resolution SS-OCT is a useful tool to guide clinical decision-making 4).
Kundan S et al. (2025) reported the combination of descemetopexy (C₃F₈ or SF₆) with corneal venting incisions in 5 cases of DMD after cataract surgery. Good visual recovery was achieved within one week in 4 cases. They suggest that elimination of residual fluid in the pre-Descemet space contributes to early DM reattachment 5).
Sharma A et al. (2023) reported double bubble pneumodescemetopexy for rolled DMD. This highly controlled technique uses a small bubble to unroll the DM and a large bubble to reattach it, avoiding corneal endothelial transplantation 1).
Hasan SM et al. (2021) achieved complete reattachment with partial descemetorhexis after failed air and SF₆ descemetopexy for late-onset DMD 45 years after penetrating keratoplasty. They proposed a tractional mechanism and showed that releasing traction is key to treatment 6).
Sharma A, Sharma R, Kulshreshta A, Nirankari VS. Double bubble pneumo-descemetopexy for the management of Descemet membrane detachment: An innovative technique. Indian J Ophthalmol. 2023;71(5):2234-2236. doi:10.4103/ijo.IJO_1623_22. PMID:37202957; PMCID:PMC10391505.
Orejudo de Rivas M, Martínez Morales J, Pardina Claver E, Pérez García D, Pérez Navarro I, Ascaso Puyuelo FJ, et al. Descemet’s Membrane Detachment during Phacocanaloplasty: Case Series and In-Depth Literature Review. Journal of clinical medicine. 2023;12(17). doi:10.3390/jcm12175461. PMID:37685527; PMCID:PMC10488042.
Bevara A, Murthy SI. Iatrogenic Descemet membrane detachment in the donor lenticule during Descemet stripping automated endothelial keratoplasty. BMJ case reports. 2023;16(12). doi:10.1136/bcr-2023-256380. PMID:38050390; PMCID:PMC10693850.
Köppe MK, Khoramnia R, Auffarth GU, Augustin VA. Pseudophakic corneal edema caused by Descemet membrane detachment using high-resolution swept-source OCT imaging. GMS ophthalmology cases. 2024;14:Doc12. doi:10.3205/oc000244. PMID:39385767; PMCID:PMC11462704.
Kundan S, Sahu PK, Sharma A, Das GK, Aamir PA. Descemet Membrane Detachment Assessed by Anterior Segment-Optical Coherence Tomography and Managed With Descemetopexy and Corneal Venting Incision: A Case Series. Cureus. 2025;17(6):e86631. doi:10.7759/cureus.86631. PMID:40709136; PMCID:PMC12287622.
Hasan SM, Jakob-Girbig J, Pateronis K, Meller D. Partial descemetorhexis for delayed Descemet membrane detachment following penetrating keratoplasty, suggestion of a pathomechanism. American journal of ophthalmology case reports. 2021;22:101077. doi:10.1016/j.ajoc.2021.101077. PMID:33898858; PMCID:PMC8056220.
Das AK, Panigrahi A, Gupta N. Central and bullous Descemet membrane detachment during cataract wound hydration: an insightful complication in a post-DALK eye. BMJ Case Rep. 2022;15(3):e249260. doi:10.1136/bcr-2022-249260.
Turaga K, Kalary J, Velamala IP. Descemet’s membrane detachment after Nd:YAG laser iridotomy in a patient with pseudoexfoliation. BMJ Case Rep. 2022;15(2):e246071. doi:10.1136/bcr-2021-246071.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.