
Milkweed Corneal Toxicity
Key points at a glance
Section titled “Key points at a glance”1. What is milkweed corneal toxicity?
Section titled “1. What is milkweed corneal toxicity?”Plants of the genus Asclepias are commonly called milkweed because of their milky sap (latex). They produce colorful flowers and play an important role in the life cycle of monarch butterflies, so they are often grown in home gardens.
When this sap comes into contact with the eye, it causes an inflammatory reaction and corneal edema. The main mechanisms of injury are carelessness during gardening or children’s contact with the plant 1). Case reports have been described for several species, including Asclepias curassavica, A. tuberosa, A. physocarpa (Gomphocarpus physocarpus), and A. fruticosa. Similar ocular toxicity has also been reported for related plants of the genus Calotropis (Sodom apple) 2-5).
Because patients may not be aware of the causal relationship between plant exposure and eye symptoms, it is necessary to consider the possibility of plant exposure in patients presenting with corneal edema 2).
Cardenolides, cardiac glycosides found in milkweed sap, inhibit Na+/K+-ATPase (sodium-potassium pump) in corneal endothelial cells. When the pump function of the corneal endothelium is impaired, water drainage from the cornea decreases, leading to corneal edema 2,3). This mechanism of action is similar to the pharmacological action of digitalis preparations.
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”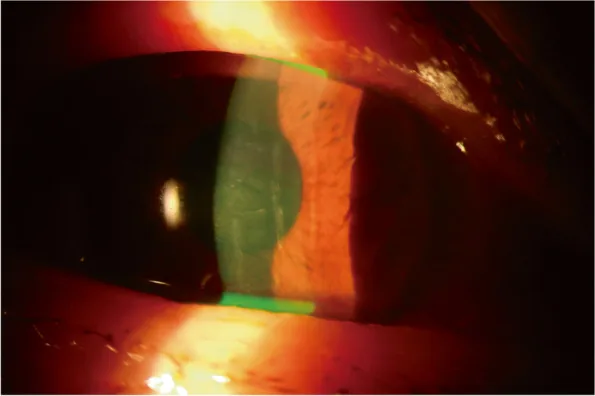
Subjective symptoms
Section titled “Subjective symptoms”After contact of the sap with the ocular surface, eye pain, redness, tearing, and decreased vision (blurred vision) occur. Symptoms appear soon after contact 1,2).
Clinical Findings
Section titled “Clinical Findings”- Decreased vision: In some cases, best-corrected visual acuity may decrease to 20/400, and in a consecutive series of 29 eyes exposed to Calotropis procera, 86% presented with visual acuity less than 20/60 at the initial visit 4).
- Conjunctival injection: Moderate injection is observed.
- Corneal edema: Corneal opacity occurs due to swelling of the corneal stroma. Central corneal thickness has been reported to increase from approximately 560 μm in the healthy eye to 727–750 μm in the affected eye 2,3). If corneal endothelial damage is mild, only stromal edema is present; if severe, epithelial edema accompanies.
- Descemet’s membrane folds: Observed in association with corneal edema.
- Decreased corneal endothelial cell density: At 3–6 months after exposure, an average reduction of approximately 18.6±9.9% in endothelial cells compared to the contralateral healthy eye may persist 4).
Severe ocular toxicity signs may include the following, but are uncommon 2,5):
- Perilimbal whitening
- Anterior chamber inflammation (anterior uveitis)
- Symblepharon
Intraocular pressure is usually within the normal range.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”The cause is direct ocular surface exposure to the milky sap (latex) of plants from the genera Asclepias or Calotropis.
- Gardening work: Sap splashes into the eye during pruning or weeding.
- Children’s contact: Inadvertent contact with plants, transferring sap to the eyes via hands.
- Not wearing protective glasses: Failure to use eye protection during work.
4. Diagnosis and examination methods
Section titled “4. Diagnosis and examination methods”Diagnosis is based on clinical findings and history of plant exposure. Since patients (especially children) may not be aware of the association between plant contact and symptom onset, actively inquire about possible plant exposure in patients presenting with corneal edema1,2).
- Slit-lamp microscopy: Evaluate corneal edema, Descemet’s membrane folds, and anterior chamber inflammation.
- Specular microscopy: Assess the degree of corneal endothelial cell damage. Endothelial cell density transiently decreases in the acute phase, but in mild cases it remains above 2,000 cells/mm² and recovers within two weeks5).
- Pachymetry (corneal thickness measurement): Useful for quantitative assessment of corneal edema3).
Differential diagnosis
Section titled “Differential diagnosis”Any disease presenting with corneal edema and conjunctival hyperemia should be considered in the differential diagnosis.
- Chemical trauma (acid or alkali)
- Viral conjunctivitis
- Herpetic keratitis
- Acute angle-closure glaucoma
- Anterior uveitis
- Trauma
5. Standard Treatment
Section titled “5. Standard Treatment”As with other ocular chemical injuries, removal of the causative agent and stabilization of the anterior segment are prioritized.
- Eye irrigation: Immediately perform thorough irrigation with normal saline. Confirm normalization by measuring ocular surface pH 1,2)
- Steroid eye drops: Prednisolone acetate 1% (6–8 times daily) or dexamethasone 0.1% eye drops are used 2,3). They upregulate Na+/K+-ATPase activity in the corneal endothelium and promote recovery of the corneal pump function.
- Hypertonic saline: Use 5% sodium chloride eye drops in combination. It reduces corneal edema through osmotic effect.
- Severe cases: There are reports of adding cyclosporine 0.1% eye drops or oral prednisolone (30 mg/day for 3 days) 3)
Daily monitoring through clinical examination is necessary until clinical stability is achieved. In a consecutive series of 29 eyes exposed to Calotropis procera, 93% (27 eyes) recovered completely within an average of 6.7 ± 2.7 days (range 3–14 days), and 90% achieved a final best-corrected visual acuity of 20/20 4). In Asclepias curassavica cases, complete recovery from visual acuity 20/60 to 20/20 was obtained within 2 weeks 3).
The prognosis is good. With appropriate irrigation and treatment with steroid eye drops and hypertonic saline, most patients recover within a few days to 2 weeks without sequelae 3,4). However, in severe cases, about 18% of corneal endothelial cell loss may persist at 3–6 months after exposure, so long-term follow-up with specular microscopy is recommended 4).
6. Pathophysiology and Detailed Mechanism
Section titled “6. Pathophysiology and Detailed Mechanism”The sap of milkweed plants contains cardenolides, cardiac glycosides. Cardenolides are compounds with a C23 steroid skeleton, similar in structure to digitalis (Digitalis), and have the property of binding to the α-subunit of Na+/K+-ATPase 2). In Calotropis procera, cardenolides such as calotropin, calotoxin, calcilin, and gigantin have been identified 4).
Corneal endothelial cells maintain corneal transparency by actively pumping water from the corneal stroma into the aqueous humor via Na+/K+-ATPase-mediated active transport (pump function). When cardenolides inhibit Na+/K+-ATPase, the pump function of the corneal endothelium decreases, leading to water accumulation in the corneal stroma and corneal edema 2,3). Cardenolides in the sap penetrate the corneal stroma without causing significant damage to the corneal epithelium and reach the endothelial layer, so the corneal epithelium is often preserved while only endothelial dysfunction becomes apparent 2).
Ocular toxicity from digitalis glycosides also involves Na+/K+-ATPase inhibition in its pathogenesis, sharing a common pathophysiological basis with milkweed corneal toxicity. However, digitalis primarily causes toxicity to photoreceptors (cone cells) via systemic administration, whereas milkweed directly damages the corneal endothelium through local exposure. In severe cases, inflammatory pathways (histamine in latex, histamine release from mast cells, prostaglandin production via cyclooxygenase-2) are also thought to play a supplementary role 4).
Steroids (dexamethasone) are effective in treatment because they upregulate Na+/K+-ATPase activity in the corneal endothelium and promote recovery of the inhibited pump function.
References
Section titled “References”-
Yang JF, Beal CJ. Corneal Toxicity Secondary to Latex From Asclepias curassavica in a Pediatric Patient. Cornea. 2021;40(12):1607-1609. doi:10.1097/ICO.0000000000002708. PMID: 34749380.
-
Mikkelsen LH, Hamoudi H, Gül CA, Heegaard S. Corneal Toxicity Following Exposure to Asclepias Tuberosa. Open Ophthalmol J. 2017;11:1-4. doi:10.2174/1874364101711010001. PMID: 28400886; PMCID: PMC5362972.
-
Lee YJ, Han SB, Hyon JY. Corneal endothelial dysfunction caused by Asclepias curassavica in a young farmer. Am J Ophthalmol Case Rep. 2019;16:100564. doi:10.1016/j.ajoc.2019.100564. PMID: 31692682; PMCID: PMC6806376.
-
Basak SK, Bhaumik A, Mohanta A, Singhal P. Ocular toxicity by latex of Calotropis procera (Sodom apple). Indian J Ophthalmol. 2009;57(3):232-234. doi:10.4103/0301-4738.49402. PMID: 19384022; PMCID: PMC2683444.
-
Ono T, Kinoshita K, Iwasaki T, Mori Y, Nejima R, Nakamura Y, Amano S, Aihara M, Miyata K. Clinical Courses Of Corneal Endothelial Dysfunction Due To Gomphocarpus physocarpus Milky Latex-Induced Injury: A Case Series. Clin Ophthalmol. 2019;13:2293-2299. doi:10.2147/OPTH.S230009. PMID: 31819354; PMCID: PMC6878928.