Dose dependency
Daily dose: The RR was 2.71 for patients taking more than 100 mg/day, compared to 1.69 for those taking 100 mg/day or less
Cumulative dose: Patients with higher lifetime cumulative doses tend to have lower endothelial cell density

Amantadine is an NMDA-type glutamate receptor antagonist, originally developed as a prophylactic agent for influenza A. It is currently used to treat tremor associated with Parkinson’s disease (PD), levodopa-induced dyskinesia, and fatigue in multiple sclerosis (MS).
A rare side effect of this drug is bilateral corneal edema. In a literature review of 33 cases, 70% of patients were women, with a median age of 52 years 1). A two-year surveillance study by the Veterans Health Administration found corneal edema in 0.27% of patients taking amantadine. A longitudinal study in Taiwan reported a relative risk (RR) of 1.98 for corneal edema with amantadine use in PD patients.
Similar corneal edema has been reported with other dopamine agonists such as methylphenidate, ropinirole, and bupropion. In all cases, recovery occurred after discontinuation, and concomitant use of multiple dopamine agonists may increase risk due to additive effects.
The main symptom is slowly progressive bilateral blurred vision over weeks to months. Onset often occurs weeks to months after starting the drug, but cases have been reported years after treatment initiation 1). In a literature review, the median visual acuity at onset was 20/200 (worse eye) 1).
The following risk factors for amantadine toxicity have been reported.
Dose dependency
Daily dose: The RR was 2.71 for patients taking more than 100 mg/day, compared to 1.69 for those taking 100 mg/day or less
Cumulative dose: Patients with higher lifetime cumulative doses tend to have lower endothelial cell density
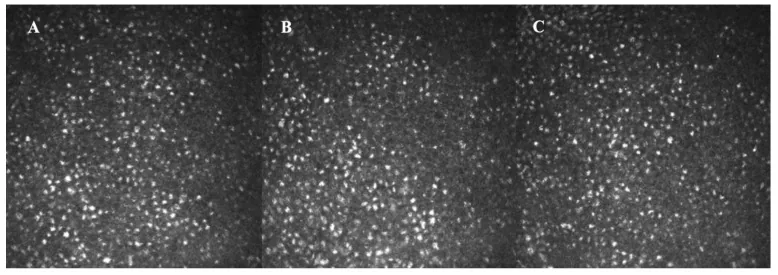
Chronic effects on the endothelium
Prospective study: Patients taking amantadine had a greater annual decrease in corneal endothelial cell density (1.51%/year) compared to non-medicated PD patients (0.94%) and healthy individuals (0.55%)
Higher doses have greater effect: The decrease in hexagonality and increase in coefficient of variation increased in a dose-dependent manner
The diagnosis of amantadine-induced corneal edema is made clinically. After excluding other causes of corneal edema, the association with amantadine use is confirmed.
In Fuchs endothelial corneal dystrophy, specular microscopy or slit-lamp microscopy characteristically reveals corneal guttata, whereas amantadine-induced corneal edema does not show guttata. Additionally, Fuchs is chronic and progressive, but amantadine-induced edema often resolves after discontinuation of the drug.
The mainstay of treatment is prompt discontinuation of amantadine. In a literature review, the majority of cases showed resolution of corneal edema within 30 days (median 30 days, interquartile range 14–35 days) after drug cessation, with visual acuity recovering to a median of 20/25 1). Coordinate with the attending neurologist to consider switching to an alternative medication.
Hypertonic saline (5% sodium chloride) eye drops may be used as symptomatic treatment for corneal edema. However, since the underlying issue is endothelial dysfunction, the effect is limited. If it progresses to bullous keratopathy, bandage contact lenses for pain management and prophylactic antibiotic eye drops may be used.
In a literature review, corneal transplantation was required in 5 of 33 cases (10 eyes) 1). Descemet membrane endothelial keratoplasty (DMEK) or Descemet stripping automated endothelial keratoplasty (DSAEK) may be selected. There are reports of non-immune graft failure if corneal transplantation is performed while continuing amantadine use, so the drug should be discontinued before transplantation.
The exact mechanism is unknown, but dose-dependent toxicity to corneal endothelial cells is considered the main cause. Corneal endothelial cells have a pump function that removes water from the corneal stroma into the anterior chamber via ion transporters such as Na⁺-K⁺ ATPase and SLC4A11, as well as a barrier function through tight junctions. These functions maintain constant corneal hydration and transparency.
Histopathological examination of cases requiring corneal transplantation for amantadine-induced corneal edema revealed moderate to complete loss of corneal endothelial cells without guttata or inflammation. It is presumed that drug-induced stress on corneal endothelial cells, when exceeding a threshold, leads to progressive endothelial dysfunction and loss, and the resulting decrease in pump function causes fluid accumulation in the corneal stroma, leading to edema.
Dose-dependent chronic toxicity is considered the main mechanism rather than an idiosyncratic reaction (onset within 1 month of starting the drug). A literature review found that only 9.7% of cases developed within 1 month 1).
Human corneal endothelial cells have little regenerative capacity; damaged cells are compensated by flattening and enlargement of surrounding cells. Even after corneal edema resolves upon discontinuation of amantadine, endothelial cell density often remains low, posing a risk of future corneal decompensation. Therefore, long-term follow-up is recommended.