Interface fluid syndrome (IFS) is a rare but vision-threatening complication after LASIK, in which fluid accumulates between the flap and the corneal stromal bed (the interface). Since early reports, it has been described as pressure-induced interlamellar stromal keratitis (PISK) associated with elevated intraocular pressure1).
The main cause of IFS is steroid-induced elevation of intraocular pressure1)3). Steroid-induced ocular hypertension causes fluid accumulation in the interface, which can also lead to underestimation of intraocular pressure3). It often occurs in the early postoperative period (days to weeks), but late-onset cases occurring 10 years after LASIK have also been reported 1).
In addition to LASIK, IFS can also occur after SMILE (small incision lenticule extraction) or lamellar keratoplasty. The incidence of IFS after LASIK in Egypt has been reported as 2.9%, but since that study used potent steroids (dexamethasone), the general incidence is presumed to be much lower.
Patients present with blurred vision as the main complaint days to months (sometimes years) after LASIK. It may be accompanied by pain or photophobia1). Typically, it occurs in patients who have used topical steroids for a long period after LASIK 1).
Decreased visual acuity: Ranges from mild reduction to hand motion. In case reports, corrected visual acuity has decreased to 20/80 1).
Elevated intraocular pressure: True intraocular pressure is elevated, but Goldmann applanation tonometry over the central cornea may show falsely low values 2). This is because the fluid cushion at the interface is easily compressed 1).
Peripheral measurement: Intraocular pressure should be measured peripherally using a Tono-Pen or dynamic contour tonometer 2).
Corneal Findings
Interface haze: Diffuse haze between the flap and stromal bed is observed1).
Fluid accumulation: A clear fluid layer may be visible on slit-lamp examination. It is not always distinct.
Corneal edema: Subepithelial edema or microbulae (microblisters) may be present1).
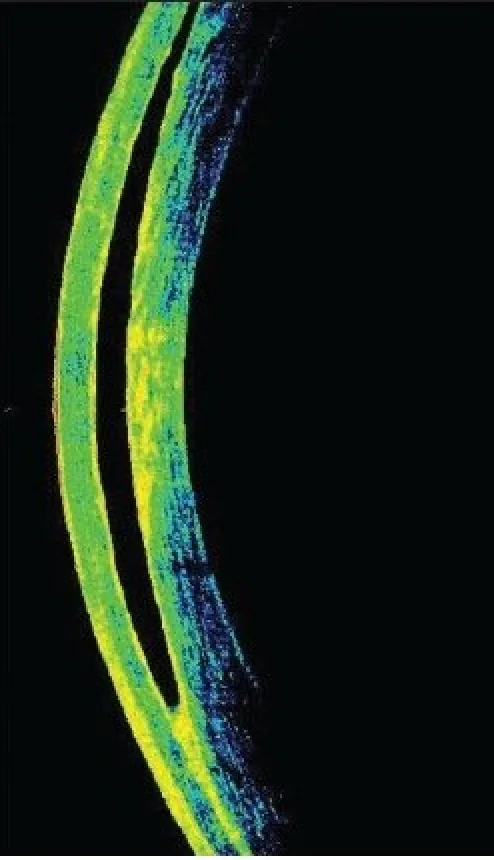
OCT findings: Anterior segment OCT can clearly confirm fluid accumulation at the interface, which is useful for definitive diagnosis1)2).
The causes of IFS are broadly classified into two categories. The first is steroid-induced intraocular pressure elevation, which is the most common cause1)3). The second is corneal endothelial dysfunction.
Any condition that causes elevated intraocular pressure can lead to IFS. Reported causes include uveitis, Posner-Schlossman syndrome, cytomegalovirus endotheliitis, toxic anterior segment syndrome (TASS), trauma, and infectious keratitis. Patients with corneal endothelial insufficiency, such as Fuchs endothelial corneal dystrophy, are also at high risk.
All patients who have undergone surgery that creates a potential space between the corneal stroma and the flap are at risk for IFS. It is most common in LASIK patients, but can also occur after SMILE or lamellar keratoplasty.
Sirisha Senthil, Varsha Rathi, Chandrasekhar Garudadri Misleading Goldmann applanation tonometry in a post-LASIK eye with interface fluid syndrome 2010 Jul-Aug Indian J Ophthalmol. 2010 Jul-Aug; 58(4):333-335 Figure 1. PMCID: PMC2907040. License: CC BY.
Corneal OCT shows a band-like hyporeflective area between the LASIK flap and the stromal bed. The tomographic image demonstrates fluid accumulated at the interface lifting the flap.
Diagnosis is made based on clinical course and slit-lamp examination, and confirmed by anterior segment OCT1). OCT can confirm fluid accumulation at the interface between the flap and stromal bed 1). Corneal densitometry (corneal brightness measurement using Scheimpflug imaging) is also useful for evaluating and grading IFS 1).
Onset 2–5 days postoperatively, pain present, normal intraocular pressure
Microbial keratitis
Normal intraocular pressure, infiltrates present
Epithelial ingrowth
Normal intraocular pressure, no interface fluid
Differentiation from DLK is particularly important. DLK is treated with steroids, but administering steroids for IFS further increases intraocular pressure and worsens symptoms1). In DLK, inflammatory mononuclear cells and granulocytes are seen, whereas in IFS, no inflammatory cells are observed1).
QHow is IFS diagnosed?
A
The diagnosis of IFS is based on a history of steroid use after LASIK, onset of blurred vision, and confirmation of interface opacity on slit-lamp microscopy. Definitive diagnosis is made by confirming fluid accumulation between the flap and stromal bed using anterior segment OCT. Since central intraocular pressure measurements may show falsely low values, peripheral measurements or dynamic contour tonometry should be used. Differentiation from DLK (diffuse lamellar keratitis) is extremely important: DLK presents with pain early postoperatively and normal intraocular pressure, whereas IFS is characterized by elevated intraocular pressure.
The basic treatment for IFS is discontinuation of steroids and initiation of intraocular pressure-lowering medications1).
Beta-blockers (e.g., timolol) are first-line; if insufficient, carbonic anhydrase inhibitors and alpha-agonists are added1). In a case report, combination therapy with brimonidine 0.2%, timolol 0.5%, and dorzolamide 2.0% improved visual acuity after 36 hours1). Intraocular pressure-lowering medications are continued for 1–3 months and then tapered1).
If intraocular pressure control is insufficient with medication, surgical intervention may be necessary. There is a report of managing IFS associated with Fuchs endothelial corneal dystrophy using DMEK (Descemet membrane endothelial keratoplasty).
If epithelial ingrowth is present, the flap is lifted and mechanical removal is performed1). Application of 50% alcohol and 0.02% mitomycin C is combined to prevent recurrence1).
Timely diagnosis of IFS is extremely important to prevent permanent vision loss. If misdiagnosed as DLK and treated with steroids, IFS worsens; therefore, differentiation between the two determines the treatment strategy.1)
QHow are IFS and DLK different?
A
IFS (Interface Fluid Syndrome) and DLK (Diffuse Lamellar Keratitis) both cause opacity at the interface after LASIK, but their pathophysiology and treatment differ. DLK is an idiopathic interface inflammation occurring 2–5 days postoperatively, with pain and normal intraocular pressure, and improves with steroid eye drops. In contrast, IFS is primarily characterized by elevated intraocular pressure, and steroids worsen it. In IFS, inflammatory cells are absent, and edema is the main feature. Treatment involves discontinuing steroids and administering intraocular pressure-lowering medications.
Two main mechanisms have been proposed for the pathophysiology of IFS.
The first mechanism is fluid movement due to elevated intraocular pressure. When intraocular pressure rises, fluid moves from the high-pressure area (anterior chamber) to the low-pressure area (interface space) through the corneal endothelium. The interface created by the LASIK flap becomes a low-pressure area, causing fluid accumulation there. Steroid-induced intraocular pressure elevation is the most common trigger for this mechanism 1)3).
The second mechanism is corneal endothelial dysfunction. When the pump function of the corneal endothelium is impaired, such as in Fuchs endothelial corneal dystrophy, water drainage from the corneal stroma becomes insufficient, making fluid accumulation in the interface more likely.
In DLK, accumulation of inflammatory mononuclear cells and granulocytes is observed, whereas in IFS, inflammatory cells are absent and only edema is present 1). Confocal microscopy reveals microlacunae (microspaces), which are thought to result from stromal edema 1).
For late-onset IFS, a hypothesis has been proposed that epithelial ingrowth forms a fistula, providing a “space” for fluid to flow into the interface 1).
Steroid-induced intraocular pressure elevation causes fluid accumulation in the interface, which also leads to underestimation of intraocular pressure. Lowering intraocular pressure resolves the inflammation. 3)
QWhy does IFS occur even when intraocular pressure measurement is normal?
A
In IFS, intraocular pressure is actually elevated. However, when measuring the central cornea with a Goldmann applanation tonometer, the cushioning effect of the fluid accumulated in the interface makes the cornea easily compressible, resulting in a falsely low reading. Therefore, in patients with a history of LASIK, peripheral intraocular pressure measurement or use of a dynamic contour tonometer is recommended.
The clinical spectrum of IFS is expanding. Although traditionally considered an early postoperative complication, a case of late-onset PISK with epithelial ingrowth occurring 10 years after LASIK has been reported 1). In this case, it is speculated that epithelial ingrowth formed a fistula and promoted fluid inflow into the interface 1). Additionally, a case has been reported where PISK developed 9 years after LASIK following the addition of steroids for the treatment of uveitis1).
With the widespread adoption of SMILE, IFS after SMILE surgery has also become a complication that should be considered in the differential diagnosis. The limitations of conventional intraocular pressure measurement methods are being recognized, and the importance of screening with anterior segment OCT is emphasized 2). When unexplained visual loss or elevated intraocular pressure is observed, OCT is recommended 1).
IFS usually occurs 1 to 3 days after surgery, but can also occur several years later. Continuous intraocular pressure monitoring is important in patients with a history of LASIK who are on long-term steroid use. 1)
Vera-Duarte GR, Guerrero-Becerril J, Müller-Morales CA, Ramirez-Miranda A, Navas A, Graue-Hernandez EO. Delayed-onset pressure-induced interlamellar stromal keratitis (PISK) and interface epithelial ingrowth 10 years after laser-assisted in situ keratomileusis. American journal of ophthalmology case reports. 2023;32:101874. doi:10.1016/j.ajoc.2023.101874. PMID:38161519; PMCID:PMC10757168.
Venkataraman P, Shroff A, Prabu S, Senthilkumar N. Behind the blur: Understanding interface fluid syndrome in post-LASIK patients. Indian journal of ophthalmology. 2025;73(9):1396. doi:10.4103/IJO.IJO_399_25. PMID:40880161; PMCID:PMC12448521.