Aniridic fibrosis syndrome (AFS) is a rare complication that occurs after intraocular surgery in patients with congenital aniridia1).
A fibrous membrane forms from the rudimentary iris root and can extend to the intraocular lens, ciliary body, and anterior retina. In 2005, Tsai et al. first reported 7 eyes of 6 patients as “progressive anterior segment fibrosis syndrome after surgery in congenital aniridia”1). As of the case report by Banifatemi et al. (2024), only 19 cases have been reported worldwide1).
Congenital aniridia is a panocular disease characterized by partial to complete absence of iris tissue1).
The incidence is estimated at 1:64,000 to 1:96,0001). 90% of cases are due to mutations in the PAX6 gene (11p13), with an autosomal dominant inheritance pattern (high penetrance)1). Two-thirds of cases are familial, and one-third are sporadic1).
Congenital aniridia presents with various ocular complications in addition to iris defects.
Visual acuity is typically limited to 20/100 to 20/2001). Due to zonular weakness, intraocular lens implantation requires careful consideration.
The PAX6 gene product is adjacent to the tumor suppressor gene WT1 on chromosome 11p13, and as a contiguous gene syndrome, WAGR syndrome (Wilms tumor, aniridia, genitourinary abnormalities, intellectual disability) may occur.
QDo all patients with congenital aniridia develop aniridia fibrosis syndrome after intraocular surgery?
A
Aniridia fibrosis syndrome occurs after intraocular surgery but is a rare complication that does not develop in all cases. A systematic review of artificial iris implantation reported an incidence of 3.1%1), and the mechanism of onset is not fully understood.
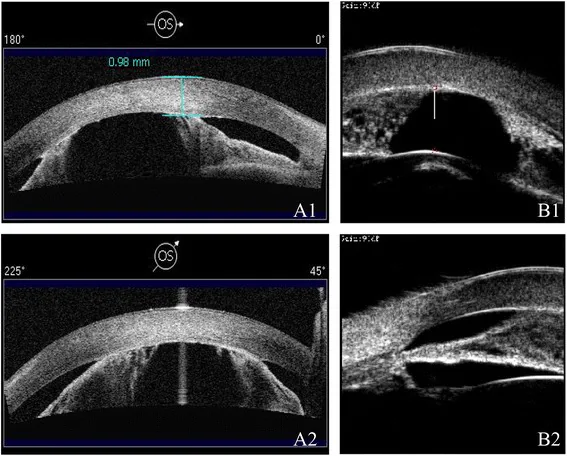
Ni W, et al. A novel histopathologic finding in the Descemet’s membrane of a patient with Peters Anomaly: a case-report and literature review. BMC Ophthalmol. 2015. Figure 2. PMCID: PMC4619091. License: CC BY.
AS-OCT (a) and UBM (b) of the left eye show a shallow anterior chamber and peripheral anterior synechiae. This corresponds to the anterior synechiae discussed in the section “2. Main Symptoms and Clinical Findings.”
The main complaint in aniridia fibrosis syndrome is painless, progressive vision loss from baseline1). Because it is painless, patients often delay seeking care. In advanced stages, observant patients may notice the presence of a membrane.
Fibrous membrane originating from the iris root: A membrane formed from the rudimentary iris root can be observed with a slit lamp. It often affects the intraocular lens.
Anterior displacement of the intraocular lens: The intraocular lens moves forward due to traction of the membrane, and in advanced cases, it contacts the cornea.
Advanced stage findings
Hypotony: Occurs when the membrane extends to cover the ciliary body. In the case reported by Banifatemi et al., the right eye had an IOP of 0 mmHg1).
Corneal endothelial failure: Ultimately leads to edema and endothelial damage of the entire cornea. In the same report, total corneal edema was observed1).
Retinal detachment: May occur when the membrane extends to the anterior retina.
In the case reported by Banifatemi et al. (a 3-year-old girl, 2 years after bilateral Ahmed glaucoma valve surgery), the following findings were noted in the right eye1):
Hypotonous eye with total corneal edema (IOP 0 mmHg)
Subluxated mature cataract superiorly and inferior zonular dehiscence
White vascular membrane extending from the rudimentary iris to the inferior part of the subluxated lens
Ultrasound biomicroscopy: thick fibrous membrane originating from the iris root extending posterior to the cataractous lens
B-scan: axial length 21 mm, optic disc edema, shallow choroidal detachment in the anterior two-thirds (no retinal detachment)
QWhy do hypotony and corneal edema occur?
A
Hypotony occurs because the fibrous membrane covers the ciliary body, impairing its function and reducing aqueous humor production1). Corneal edema is caused by corneal endothelial damage due to contact with the intraocular lens or hypotony.
The etiology of aniridia fibrosis syndrome is unknown. However, all reported cases have occurred after intraocular surgery.
Risk factors include the following:
History of intraocular surgery: Cataract extraction with intraocular lens implantation is the most common
Placement of intraocular devices: Multiple intraocular devices such as glaucoma drainage devices (tube shunts) have been associated
Female sex: 88% of reported cases were female
Multiple intraocular surgeries: In the initial report by Tsai et al., all cases had a history of multiple intraocular surgeries1)
Surgical history in 7 eyes of 6 patients by Tsai et al.1): cataract surgery with posterior chamber intraocular lens in 7 eyes, tube shunt in 6 eyes, corneal transplant in 4 eyes. In 9 cases by Bakhtiari et al.1): cataract surgery with intraocular lens implantation in all cases, tube shunt in 7 cases, corneal transplant/corneal limbal allograft in 7 cases.
Two theories have been proposed regarding the mechanism of onset.
Mechanical irritation theory: Intraocular devices touching rudimentary iris tissue or immature iris vessels provide a scaffold for membrane formation1)
PAX6 mutation-related fibrosis predisposition theory: PAX6 negatively regulates Wnt signaling, and chronic activation of Wnt signaling due to PAX6 mutation promotes fibrosis. Wang et al. confirmed in a mouse model that PAX6 haploinsufficiency induces a prefibrotic state before surgery1)
The diagnosis of aniridia fibrosis syndrome is made by clinical observation in patients with congenital aniridia who have a history of intraocular surgery.
Regular slit-lamp examination is the cornerstone of diagnosis 1). It can reveal a fibrous membrane originating from the iris root and enveloping the intraocular lens. In early stages when the cornea is clear, detailed evaluation of the anterior segment is possible.
This is an essential test when there is anterior segment media opacity such as corneal opacification 1).
Assessment of ciliary body status
Determination of the extent of the fibrous membrane
Confirmation of cyclitic membrane formation
In the report by Banifatemi et al., ultrasound biomicroscopy was performed under chloral hydrate anesthesia, revealing a thick fibrous membrane extending from the iris root to the posterior aspect of the cataractous lens 1).
The following conditions should be differentiated:
Intraocular membranes due to other causes: postoperative inflammatory membranes, peripseudophakic membranes
Postoperative inflammatory reaction: differentiation from simple postoperative inflammation (aniridia fibrosis syndrome is characterized by a paucity of inflammatory signs)
Recurrence: Recurrence was observed only in cases that underwent intraocular lens removal/exchange. Concluded that simultaneous intraocular lens removal is effective in preventing recurrence.
Visual outcomes: Visual improvement was observed in all 5 surgical cases 1).
Bakhtiari et al. (9 cases)
Surgical technique: All cases received a Boston KPro type 1 implant (primary or secondary). Intraocular lens removal was performed in 7 of 9 cases, and vitrectomy in 8 cases.
Boston type 1 keratoprosthesis is a viable treatment option not associated with recurrence of aniridia fibrosis syndrome1). Since the KPro is placed away from the iris root (the origin of the lesion), it is thought to cause less iris irritation.
However, it should be noted that retro-KPro membrane formation occurs at a high rate (61–66%) in aniridic eyes. This is significantly higher than the rate in non-aniridic eyes (26.7–39%)1), and this retro-KPro membrane may also be a phenotype of aniridia fibrosis syndrome1).
The retention rate of Boston KPro type 1 in aniridic eyes was 83.3% (mean follow-up 58.7 months) in Dyer et al. and 87% (54 months follow-up) in Shah et al.1).
Bakhtiari et al. recommend complete vitrectomy rather than limited anterior vitrectomy to prevent recurrence1).
QWhat happens to vision if surgery is not performed?
A
Outcome data for cases with a confirmed diagnosis of AFS that did not undergo surgery are limited. In the case report by Banifatemi et al. (2024), surgery was not performed due to parental refusal1). In general, without treatment, progression of corneal endothelial failure, hypotony, and retinal detachment is a concern. In the report by Tsai et al., all surgically treated cases showed visual improvement, emphasizing the importance of early intervention1).
Pathological analysis by Tsai et al. revealed the following 1):
Origin of fibrous tissue: Fibrous tissue from the rudimentary iris root
Membrane characteristics: Dense, hypocellular fibrous membrane with sparse vascularity
Immunohistochemistry: Few T cells and macrophages in 2 cases, suggesting inflammation is not the primary cause (inflammatory cells present in 1 case)
Electron microscopy: Mixture of immature collagen bundles and mature fibers. No glial cells, corneal endothelial cells, or lens epithelial cells
Banifatemi et al. (2024) state that “the fibrous membrane resembles postoperative intraocular lens membranes in chronic uveitis but differs in the absence of inflammation” 1).
This hypothesis suggests that contact between an intraocular device and rudimentary iris tissue or immature iris vessels provides a scaffold for membrane formation 1). This is consistent with the clinical observation that aniridia fibrosis syndrome occurs in association with various intraocular devices such as intraocular lenses, tube shunts, and artificial irises.
PAX6 is a transcription factor that negatively regulates Wnt signaling. This hypothesis proposes that chronic upregulation of Wnt signaling due to PAX6 mutation creates a predisposition to intraocular fibrosis 1). Wang et al. demonstrated in a mouse model that PAX6 haploinsufficiency (haploPAX6) induces a prefibrotic state even in unoperated eyes compared to wild-type 1).
Similar progressive fibrosis has been reported in other congenital anterior segment anomalies such as Peters anomaly, suggesting that PAX6 mutations are broadly associated with a fibrotic predisposition 1).
7. Latest Research and Future Prospects (Reports at the Research Stage)
The rate of retroprosthetic membrane formation after Boston KPro type 1 implantation in aniridic eyes is 61–66%, significantly higher than in non-aniridic eyes (26.7–39%) 1).
Yang et al. have pointed out that this high rate of retroprosthetic membrane formation may be a phenotype of aniridia fibrosis syndrome 1). Meanwhile, Muzychuk et al. reported that aniridia is a significant risk factor for vision loss after Boston KPro surgery 1).
Artificial Iris Implantation and Aniridia Fibrosis Syndrome
In a systematic review of artificial iris implantation by Romano et al., the incidence of aniridia fibrosis syndrome was reported to be 3.1% in a study of 96 eyes with aniridia by Figueredo and Snyder 1). Since artificial iris implantation functions as an intraocular device similar to intraocular lenses and tube shunts, it carries a potential risk of developing aniridia fibrosis syndrome.
Molecular Mechanism Research of Aniridia Fibrosis Syndrome
Wang et al.’s mouse model study is one of the first systematic studies to elucidate the molecular mechanisms of aniridia fibrosis syndrome 1). Selective inhibition of the Wnt signaling pathway has been suggested as a potential future therapeutic target, but it has not yet reached clinical application.
Banifatemi M, Razeghinejad R, Salouti R, Abolfathzadeh N. Aniridic fibrosis syndrome in a child with Ahmed glaucoma valve: Report of a case and review of the literature. J Curr Ophthalmol. 2024;36:453-6. doi:10.4103/joco.joco_155_24.
Bakhtiari P, Chan C, Welder JD, de la Cruz J, Holland EJ, Djalilian AR. Surgical and visual outcomes of the type I Boston Keratoprosthesis for the management of aniridic fibrosis syndrome in congenital aniridia. Am J Ophthalmol. 2012;153(5):967-971.e2. PMID: 22265154.
Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, et al. PAX6-Related Aniridia. . 1993. PMID: 20301534.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.