An iris cyst is a general term for a cystic structure containing fluid that forms within the iris or on its surface.
Epidemiology and classification overview
Iris cysts are broadly classified into primary and secondary types. Primary cysts include iris pigment epithelium (IPE) cysts and stromal cysts, while secondary cysts include implantation cysts after trauma or surgery, and drug-induced cysts. Among primary cysts, stromal cysts account for 11% of all iris cysts. 3)
Secondary cysts in adults often result from trauma or intraocular surgery. Rapidly enlarging cysts in children and young adults are mostly stromal cysts. Posterior pigment epithelial cysts are more common, usually small and asymptomatic, requiring no treatment.
Familial pigment epithelial cysts
Familial cases have been reported. In one family, 8 members across 3 generations presented with bilateral pupillary margin IPE cysts, confirming an autosomal dominant inheritance pattern. 4) This condition has been associated with ACTA2 and MYH11 mutations (familial thoracic aortic aneurysm and dissection; FTAAD), and cardiovascular evaluation is recommended. 4)
QAre iris cysts malignant?
A
Iris cysts are almost always benign lesions. However, differentiation from iris melanoma or solid tumors may be necessary, and UBM or anterior segment OCT can be used to examine internal structure. If there are no features suspicious for malignancy (solid components, pigmentation, abnormal vessels), most cases can be managed with observation.
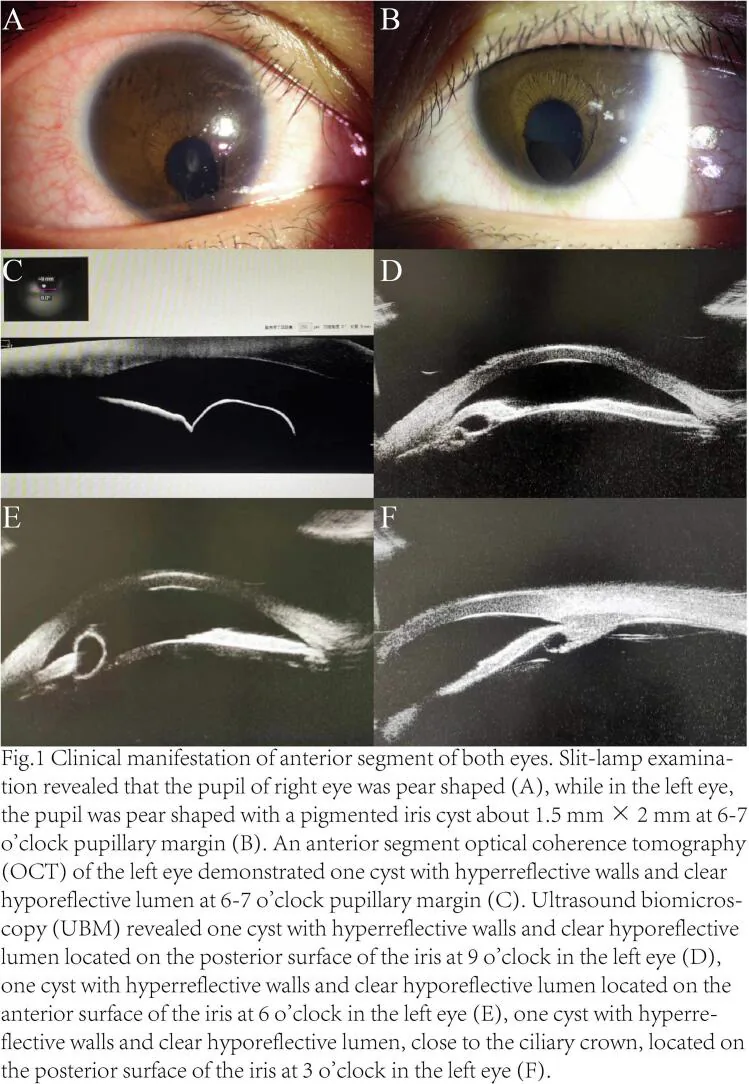
Slit-lamp photograph and anterior segment tomographic image of an iris cyst
Song XZ, et al. Congenital bilateral coloboma of iris and choroid accompanied by unilateral multiple primary pigmented iris cysts: A case report. Int J Surg Case Rep. 2024. Figure 1. PMCID: PMC11615603. License: CC BY.
Slit-lamp photograph shows a small pigmented iris cyst near the pupillary margin and pupillary distortion. An anterior segment OCT/UBM-like image depicts cystic lesions around the iris, demonstrating the correspondence between clinical findings and diagnostic imaging.
Location: Typically at the pupillary margin to the posterior iris surface.
Appearance: Translucent to brownish smooth cyst wall. Results from separation of the two layers of pigment epithelium.
Characteristics: Often small and stable.
Stromal Cyst
Location: Within the iris stroma.
Appearance: Filled with clear to turbid fluid. Contains mucin-producing cells from ectopic ectodermal origin.
Complications: Mucogenic glaucoma (aqueous outflow obstruction due to mucoid material).
Secondary (epithelial implantation) cyst: Occurs after trauma or surgery. Rapidly enlarges, may cause corneal endothelial damage and glaucoma. UBM shows a thin, hyperechoic wall. 2)
Corneal endothelial damage: Large cysts contacting and compressing the corneal endothelium can cause corneal edema and endothelial cell damage. In a report of a 58-year-old male, the cyst occupied one-third of the anterior chamber volume and directly contacted the endothelium, with corrected visual acuity reduced to 0.3. 1)
Free-floating in the anterior chamber: Pigment epithelial cysts may become free-floating in the anterior chamber and be observed as freely floating cysts. 9)
QHow can iris cysts be differentiated from iris melanoma?
A
Slit-lamp examination reveals the cyst’s transparency and smooth surface; UBM or anterior segment OCT confirms internal fluid components. Pigmentation, solid components, abnormal vascular proliferation, or rapid growth are signs suspicious for malignancy. Evaluation of internal blood flow with high-frequency color Doppler helps in differentiation.
Trauma/perforating injury: Epithelial cells enter the anterior chamber through the wound and proliferate.
After intraocular surgery: Occurs after cataract surgery, corneal transplantation, etc. There are case reports of cyst development up to 24 years after trauma. 2)
Long-term use of miotics and prostaglandin drugs: Risk of drug-induced cysts.
Standard diagnostic method, most useful for differentiating from solid tumors. A 50 MHz ultrasound probe confirms a thin-walled cyst filled with fluid within the iris stroma. 3)
Joshi et al. (2022) reported that in a case of congenital bilateral stromal cyst (1 month old), UBM (50 MHz) visualized a thin-walled, echolucent cyst and was useful in excluding a solid tumor. 3)
Angle narrowing, maximum iris thickness, ciliary body thickness, IPE posterior bowing, and anterior displacement are also evaluated.
Used as a supplementary test to UBM. Shows a pattern of high reflectivity of the cyst wall and low reflectivity of the lumen. 9)
Ho et al. reported that in free IPE cysts, AS-OCT showed a hyperreflective wall and hyporeflective lumen, and the optical density of the cyst fluid measured by ImageJ was equivalent to that of intraocular fluid (21.5). 9)
Cytology of the aspirate aims to exclude malignancy. In fibrin tissue specimens, non-keratinized stratified squamous epithelium (traumatic cyst) or cuboidal epithelium (pigment-containing macrophages) are observed. 8)
QWhich is superior, UBM or anterior segment OCT?
A
UBM is recommended as a standard examination because it can visualize the posterior pole (ciliary body and angle). Anterior segment OCT is non-invasive, easy to repeat, and suitable for follow-up. Ideally, both should be used complementarily.
Small, asymptomatic primary pigment epithelial cysts are managed with observation. Even after 10 years of follow-up, spontaneous regression or stability is common.
Nd:YAG laser: Aims to collapse the cyst by perforating its wall. Effective for small cysts, but recurrence rate is high for large cysts. In familial IPE cysts (3 generations), a single shot of 0.3–1.0 mJ resulted in no recurrence for 9 months. 4) In two sibling cases, Nd:YAG laser (1.0 mJ) maintained stability for 2 years. 10)
Argon laser: Sometimes used for stromal cysts and postoperative cysts.
Diode endolaser photocoagulation: A report describes 196 spots, 215 mW, 50 ms irradiation under anterior segment endoscopy, followed by excision of the anterior cyst wall with a vitreous cutter. 1)
Aspirate and collapse the cyst contents using a 30G needle. Adjuvant therapy is needed to prevent recurrence.
Absolute ethanol perfusion: An established method that destroys the epithelium by injecting into the cyst cavity. Challenges include difficulty in commercial availability and toxicity.
Mitomycin C (MMC) injection: A triple therapy combining aspiration, mitomycin C (0.0002 mg/mL, 5 minutes) injection, anterior wall resection with a vitreous cutter, and posterior wall cauterization has been reported. Two 1-mm incisions without iridectomy, no recurrence at 6 months. 5)
Fibrin glue injection (TISSEEL VH): After aspiration, inject fibrinogen and diluted thrombin (1:10) into the cyst cavity to adhere the cyst wall. A 61-year-old male (cyst 4.20×7.56×8.22 mm) showed visual improvement from 20/200 to 20/30, no recurrence at 3 months. 6)
Visco-dissection + cystectomy + sector iridectomy: Used for large cysts and infant cases (bilateral cysts at 1 month of age). 3)
Trypan blue-assisted excision: 27G needle aspiration → 0.06% trypan blue injection for 40 seconds (staining visualization) → excision with forceps + 23G vitreous cutter. No recurrence at 7 days postoperatively. 7)
Fibrin glue-assisted pediatric excision (miOCT-guided): Aspiration of 2/3 volume with 31G needle → injection and hardening of fibrin glue (0.04 mL) → en bloc excision. No recurrence at 2.5 years and 3 months in two infants (6 months and 3 months old). Pathology: stratified non-keratinized squamous epithelium (case 1), cuboidal epithelium with pigment-containing macrophages (case 2). 8)
Simultaneous DMEK: In cases with advanced corneal endothelial damage due to the cyst, diode endolaser photocoagulation + vitreous cutter excision + DMEK transplantation were performed in one stage, with no recurrence at 6 months and improvement of BCVA to 20/25. 1)
QCan cyst aspiration alone cure the condition?
A
Aspiration alone leaves epithelial cells on the cyst wall, leading to a high recurrence rate. To prevent recurrence, combining anhydrous ethanol perfusion, mitomycin C injection, fibrin glue, or laser photocoagulation is recommended.
It occurs due to dissociation of the two layers of pigment epithelium (anterior and posterior) at the posterior part of the iris. Fluid accumulates between the dissociated layers, forming a cyst.
It originates from ectodermal rest. The inner wall contains mucus-producing cells, and the secreted mucus (mucopolysaccharide) can obstruct the aqueous outflow pathway, leading to mucogenic glaucoma.
Conjunctival or corneal epithelial cells enter the anterior chamber through trauma or surgical wounds, proliferating and enlarging. As it progresses, it extensively covers the corneal endothelium, iris, and angle, causing refractory glaucoma and corneal endothelial failure. Since the implanted cells retain functional epithelial secretory ability, the cyst continues to enlarge.
ACTA2 (α-smooth muscle actin) and MYH11 (smooth muscle myosin heavy chain) mutations cause smooth muscle dysfunction. Reduced function of these proteins expressed in the smooth muscle of the iris sphincter and dilator muscles is thought to promote cyst formation. 4)
Regarding pigment epithelial cysts of the pupillary margin (so-called flocculi), the risk of aortic events in ACTA2 mutation carriers is estimated to reach 75% by age 85, and cardiovascular screening is strongly recommended. 4)
A shift from conventional surgical resection to more tissue-preserving techniques is underway.
Duphare et al. (2022) performed fibrin glue-assisted aspiration for a large postoperative stromal cyst (4.20×7.56×8.22 mm) and reported no recurrence and visual acuity of 20/30 at 3 months. Fibrin glue is considered a promising alternative to absolute ethanol or sclerosing agents. 6)
Arnold et al. (2022) performed a single-stage surgery combining diode endolaser photocoagulation, 25-gauge vitreous cutter excision, and DMEK transplantation for a recurrent iris cyst complicated by corneal endothelial dysfunction. At 6 months postoperatively, there was no cyst recurrence and corrected visual acuity was 20/25. 1)
Rashid et al. (2025) reported miOCT-guided fibrin glue-assisted en bloc resection in infant cases (aged 6 months and 3 months). This novel technique enables complete block resection while confirming fibrin glue filling within the cyst using intraoperative OCT, with no recurrence observed for up to 2.5 years. 8)
The association between familial pigment epithelial cysts and ACTA2/MYH11 gene mutations is becoming clearer. 4) Some experts recommend genetic testing, cardiovascular evaluation, and family screening for all cases. Establishment of systematic screening programs for gene mutation carriers is expected in the future.
Quantification of cyst fluid optical density using ImageJ analysis of anterior segment OCT may be applied to evaluate the nature of the fluid content (distinguishing intraocular fluid from mucus). 9)
Arnold S, Kim E, Derivaux D, Parker JS, Parker JS. DMEK with endophotocoagulation and cyst wall removal for corneal endothelial decompensation due to iris cyst. Am J Ophthalmol Case Rep. 2022;26:101417.
Cabezos I, García-Monge L, Domínguez-Serrano M. Implantation iris cysts developing 24 years after penetrating keratoplasty. Am J Ophthalmol Case Rep. 2022;25:101275.
Joshi A, Barman NR, et al. Bilateral congenital stromal iris cyst presenting with secondary glaucoma. Am J Ophthalmol Case Rep. 2022;25:101237.
Jiang A, Liang L, She K, Lu F. Multimodal optical imaging of iris flocculi in three consecutive generations: a case report. Front Med (Lausanne). 2024;11:1369884. doi:10.3389/fmed.2024.1369884. PMID:39267980; PMCID:PMC11390461.
[著者名不明]. Triple treatment therapy for iris cyst: aspiration, mitomycin-C injection, and vitrectomy cutter excision. Int Ophthalmol. 2024.
Duphare C, Ambati NR, Shildkrot Y. Tissue glue for management of large iris cyst. Am J Ophthalmol Case Rep. 2022;28:101742.
[著者名不明]. Trypan blue-assisted iris cyst excision for corneal endothelial decompensation. Case report. 2024.
Rashid MHO, et al. Fibrin glue-assisted en bloc excision of iris cysts in pediatric patients with miOCT guidance. J AAPOS. 2025.
Oli A, Waikar S, Malik R, Bhirud R. Optical Coherence Tomography and ImageJ Software for objective assessment of optical density of anterior chamber iris cyst. Rom J Ophthalmol. 2021;65(3):255-258. doi:10.22336/rjo.2021.50. PMID:35036646; PMCID:PMC8697790.
[Authors]. Successful treatment of bilateral familial iris flocculi associated with aortic dissection risk. Case report. PMC12296538. 2025.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.