An add-on intraocular lens (add-on IOL; supplementary IOL, piggyback IOL) is a supplementary intraocular lens inserted in front of the existing IOL after cataract surgery. It is mainly fixed in the ciliary sulcus and aims to correct residual refractive error, presbyopia, and aberrations.
Cataract surgery has become a nearly perfected procedure with phacoemulsification and foldable IOLs via small incisions 1). As part of efforts to achieve “higher quality visual function” postoperatively, value-added IOLs such as aspheric, toric, and multifocal IOLs have been developed and approved. In this context, add-on IOLs are positioned as an option to solve postoperative refractive problems later.
1993: Gayton et al. first reported the concept of “piggyback” using two IOLs for extreme hyperopia
1999: Gayton & Sanders applied piggyback IOL for refractive correction in pseudophakic eyes2)
1999: Findl et al. analyzed the contact zone between piggyback acrylic IOLs3)
2000s: Interlenticular opacification (ILO) due to double in-the-bag implantation became a problem4)5). Dedicated add-on IOLs (HumanOptics 1stQ, Rayner Sulcoflex, etc.) were developed, significantly reducing the risk
Recent years: Variety expanded to multifocal, toric, and EDOF add-on IOLs
For residual refractive error after cataract surgery or desire for presbyopia correction, when corneal refractive surgery (e.g., LASIK) is difficult, add-on IOLs may be considered as an alternative to IOL exchange8, 9, 10). Currently, it is often performed as self-pay (out-of-pocket) treatment, and adequate explanation of costs and indications is necessary before surgery.
QIs add-on IOL covered by insurance?
A
Add-on IOLs are currently often not covered by insurance and are performed as self-pay treatment. Costs vary depending on the facility and type of IOL used, so it is necessary to check details with the medical institution before surgery.
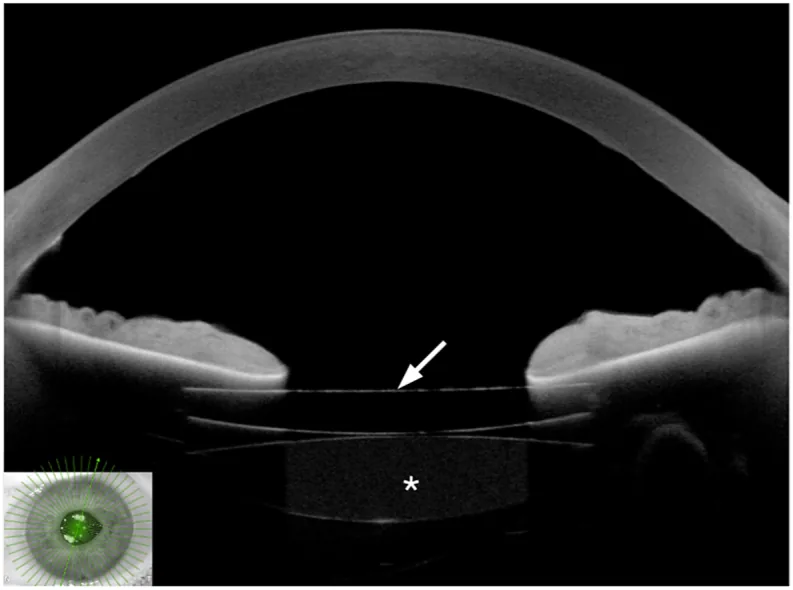
Anterior segment OCT shows an add-on intraocular lens inserted in front of the primary intraocular lens. The positional relationship between the two IOLs and the iris is visible, demonstrating the placement of the additional lens in the target patient.
The main indications for add-on IOLs are broadly divided into correction of residual refractive error and presbyopia correction.
Correction of residual refractive error (spherical and astigmatic) after cataract surgery: Since the additional power can be determined based on subjective refraction, it is easy to address spherical power deviation and astigmatic deviation.
Cases where corneal refractive surgery (e.g., LASIK) is difficult: insufficient corneal thickness, concurrent corneal disease
Presbyopia correction: adding a multifocal add-on to a monofocal IOL eye to provide near and intermediate vision
Extreme hyperopia exceeding the power range of a single IOL1)
May be considered for managing postoperative photic phenomena such as negative dysphotopsia depending on the case
Alternative refractive correction when IOL exchange is difficult (e.g., strong adhesion between the capsule and IOL)
Evaluation criteria for indications and contraindications
Multifocal IOL (in principle) and anterior chamberIOL
Corneal endothelial cells
Sufficient density
Severe corneal endothelial cell loss
QCan an add-on IOL be placed in an eye that already has a multifocal IOL?
A
Add-on IOLs are mainly intended for eyes with monofocal IOLs. Adding an add-on to an eye with a multifocal IOL may cause optical interference and is generally contraindicated. For correction of residual refractive error, corneal refractive surgery is often considered first, and the suitability of an add-on IOL requires individual evaluation by a specialist.
Dedicated add-on IOLs have the following design features.
Vault structure (posterior concave surface): The posterior surface is concave to prevent contact with the existing in-the-bag IOL and reduce the risk of ILO.
Large diameter design: The overall diameter is about 14 mm, allowing stable fixation in the ciliary sulcus (typical in-the-bag IOLs have an overall diameter of 11–13 mm).
Power determination based on subjective refraction: The power is calculated from subjective refraction rather than corneal curvature or axial length, reducing the risk of refractive error.
Power calculation for add-on IOLs differs from standard cataractIOL calculation.
Use the manifest refraction directly, adjusting for vertex distance to calculate the power.
Use online calculators provided by manufacturers (e.g., Rayner Sulcoflex Calculator).
For toric add-on IOLs, the target for correction is the residual refractive astigmatism (from manifest refraction), not the total corneal astigmatism.
QHow is the power of an add-on IOL determined?
A
The power of an add-on IOL is determined based on the stable manifest refraction after surgery. Standard cataractIOL formulas (dependent on corneal curvature and axial length) are not used; instead, the manifest refraction can be directly utilized, reducing the risk of refractive error. The power is calculated by entering the spectacle prescription into the manufacturer’s dedicated calculation tool.
Incision: 2.2–2.8 mm corneal incision (chosen according to the size of the IOL used)
Viscoelastic injection: Fill the anterior chamber with sodium hyaluronate (e.g., Healon) to create a working space that protects the existing IOL and corneal endothelium
Add-on IOL insertion: Guide the folded IOL into the anterior chamber using an injector
Fixation in the ciliary sulcus: Place the haptics in the ciliary sulcus (under the iris, in front of the existing IOL). By placing the add-on IOL in the ciliary sulcus separately from the existing in-the-bag IOL, rather than stacking two IOLs in the bag, the risk of IOL opacification is reduced 4, 5, 8, 10)
Complete removal of viscoelastic: Thoroughly aspirate all viscoelastic from the anterior and posterior chambers (residual viscoelastic can cause postoperative intraocular pressure elevation)
Wound closure: Self-sealing via stromal hydration; nylon suture if necessary
Steroid eye drops: Betamethasone 0.1% or prednisolone acetate 1% eye drops 4 times daily (tapered)
Intraocular pressure monitoring: Monitor for transient IOP elevation due to ciliary sulcus stimulation; measure on postoperative day 1 and at 1 week.
Observation schedule: Postoperative day 1, 1 week, 1 month, 3 months, and 6 months.
Postoperative refraction examination: Check refractive stability at 1 month postoperatively. If the difference from the target refraction is large, perform detailed evaluation of IOL position.
IOL exchange involves manipulation of the capsule and existing IOL, so in cases with strong adhesions, the invasiveness and risk of complications must be considered. Decreased visual function after IOL exchange has also been reported 6), and from the perspective of avoiding invasiveness to the capsule and IOL, add-on IOL may be selected.
This is a complication that tends to occur when two IOLs are inserted into the capsule, causing opacification between the two lenses and reducing vision 4)5). With the method of fixing a specially designed add-on IOL in the ciliary sulcus, the risk of occurrence is significantly reduced 1). The basic principle is the placement of one IOL in the capsule plus one add-on IOL in the ciliary sulcus.
Persistent chafing of the posterior iris surface by the haptic can cause UGH syndrome, presenting with uveitis, glaucoma, and hyphema. In specially designed add-on IOLs, the haptic diameter is optimized to reduce the risk. If elevated intraocular pressure or increased anterior chamber flare persists postoperatively, suspect this syndrome.
Acute glaucoma attack caused by obstruction of aqueous outflow between the iris and the add-on IOL. This can be prevented by performing a peripheral iridectomy during surgery.
The main cause is a mismatch between the ciliary sulcus diameter and the size of the add-on IOL. Preoperative evaluation of the ciliary sulcus diameter using anterior segment OCT or UBM helps select the appropriate size and prevent this complication.
If the anterior chamber depth is shallow, the distance between the corneal endothelium and the IOL becomes shorter, increasing the risk. Preoperatively, evaluate the anterior chamber depth and corneal endothelial cell density, and determine individually whether the conditions of the IOL to be used are suitable.
Add-on IOLs can be removed if the result is unsatisfactory or if complications occur. This reversibility is one of the important advantages over IOL exchange. Long-term outcomes depend on the IOL design, stability of ciliary sulcus fixation, and regular postoperative observation.
The following representative clinical results have been reported.
For Sulcoflex add-on IOLs, a high proportion of postoperative refraction within ±0.5 D has been reported 8)
For supplementary IOLs such as 1stQ AddOn Mono, improvement in residual refractive error has been reported 9, 10)
For toric add-on IOLs, improvement in residual astigmatism is expected with preoperative planning including axis management
Piggyback for posterior microphthalmos: refractive accuracy comparable to primary implantation 7)
QCan the add-on IOL be removed later?
A
Add-on IOLs are fixed in the ciliary sulcus and are in a position independent of the in-the-bag IOL, so they can be removed if necessary. This reversibility is one of the advantages over IOL exchange or corneal refractive surgery, which involve permanent changes. However, removal also requires surgery, and the risk of complications is not zero, so this should be explained preoperatively.
Comparison with Light Adjustable Lens (LAL): LAL is an IOL whose power can be fine-tuned postoperatively with ultraviolet irradiation, and is attracting attention as an option that can minimize residual refractive error from the time of primary implantation. It may be an alternative to add-on IOLs, but its approval status is limited in various countries.
Development of aberration-correcting add-ons: Research on custom add-on IOLs linked to wavefront aberration analysis is progressing, and it is expected to be applied to individual correction of higher-order aberrations.
EDOF-type add-on IOLs: Extended Depth of Focus add-on IOLs are under development, aiming to achieve presbyopia correction with less glare and halo than conventional multifocal add-ons.
Comparison with reverse optic capture: Comparative studies of piggyback and reverse optic capture for negative dysphotopsia have been reported, and the development of patient selection guidelines is progressing.
In determining the indication for add-on IOLs, the trend is to comprehensively evaluate the cause of residual refractive error, the position of the existing IOL, anterior chamber depth, and endothelial cell count.
Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology. 2022;129(1):P1-P126. doi:10.1016/j.ophtha.2021.10.006. PMID: 34780842.
Gayton JL, Sanders V, Van der Karr M, Raanan MG. Piggybacking intraocular implants to correct pseudophakic refractive error. Ophthalmology. 1999;106(1):56-9. doi:10.1016/S0161-6420(99)90005-2. PMID:9917781.
Findl O, Menapace R, Rainer G, Georgopoulos M. Contact zone of piggyback acrylic intraocular lenses. Journal of cataract and refractive surgery. 1999;25(6):860-2. doi:10.1016/s0886-3350(99)00031-0. PMID:10374169.
Werner L, Shugar JK, Apple DJ, Pandey SK, Escobar-Gomez M, Visessook N, et al. Opacification of piggyback IOLs associated with an amorphous material attached to interlenticular surfaces. Journal of cataract and refractive surgery. 2000;26(11):1612-9. doi:10.1016/s0886-3350(00)00485-5. PMID:11084268.
Shugar JK, Keeler S. Interpseudophakos intraocular lens surface opacification as a late complication of piggyback acrylic posterior chamber lens implantation. Journal of cataract and refractive surgery. 2000;26(3):448-55. doi:10.1016/s0886-3350(99)00399-5. PMID:10713243.
Abdalla Elsayed MEA, Ahmad K, Al-Abdullah AA, Malik R, Khandekar R, Martinez-Osorio H, et al. Incidence of Intraocular Lens Exchange after Cataract Surgery. Scientific reports. 2019;9(1):12877. doi:10.1038/s41598-019-49030-2. PMID:31501458; PMCID:PMC6733834.
Elhofi A, Helaly HA, Said A. Comparison between refractive outcome of primary piggyback intraocular lens versus secondary lens iris claw lens in posterior microphthalmos. J Ophthalmol. 2019;2019:1356982. doi:10.1155/2019/1356982. PMID: 30895155; PMCID: PMC6393898.
Falzon K, Stewart OG. Correction of undesirable pseudophakic refractive error with the Sulcoflex intraocular lens. Journal of refractive surgery (Thorofare, N.J. : 1995). 2012;28(9):614-9. doi:10.3928/1081597X-20120809-01. PMID:22947288.
Kahraman G, Amon M. New supplementary intraocular lens for refractive enhancement in pseudophakic patients. J Cataract Refract Surg. 2010;36(7):1090-1094. doi:10.1016/j.jcrs.2009.12.045. PMID: 20610084.
Khan MI, Muhtaseb M. Performance of the Sulcoflex piggyback intraocular lens in pseudophakic patients. Journal of refractive surgery (Thorofare, N.J. : 1995). 2011;27(9):693-6. doi:10.3928/1081597X-20110512-01. PMID:21598871.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.