Drug-induced uveitis is a relatively rare condition in which systemically or topically administered drugs trigger intraocular inflammation. It accounts for 0.38–1.4% of all uveitis cases 1) and less than 0.5% in tertiary referral uveitis clinics.
It became widely recognized in the 1990s following case reports of rifabutin and cidofovir in AIDS patients. 1) In recent years, reports have increased due to the widespread use of intravitreal injections, immune checkpoint inhibitors, and vaccines.
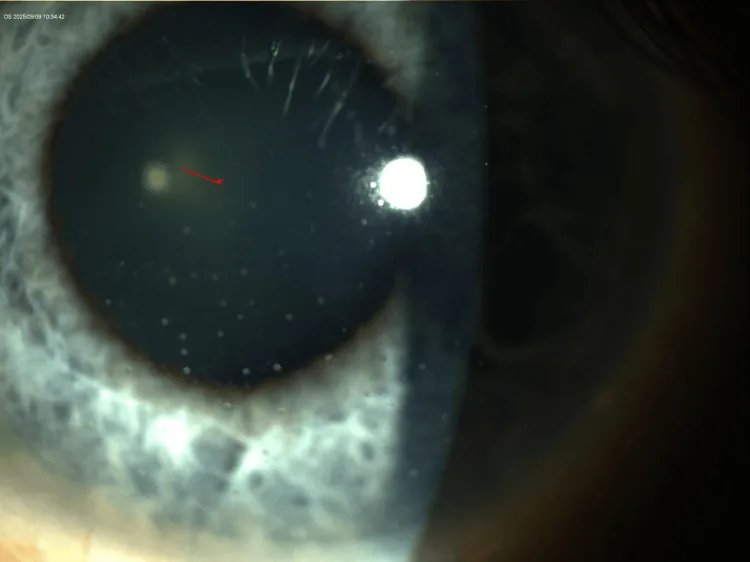
Miyashiro MJ, et al. Bilateral Granulomatous Keratic Precipitates Following Inadequate Antibiotic Coverage for Presumed Lyme Disease. Cureus. 2025. Figure 4. PMCID: PMC12669937. License: CC BY.
Slit-lamp magnified photograph of the left eye showing multiple large mutton-fat keratic precipitates clustered on the corneal endothelium, with a quiet anterior chamber and no flare or hypopyon. Corresponds to the keratic precipitates discussed in section “2. Main Symptoms and Clinical Findings.”
Depending on the causative drug, the condition can present with various manifestations, from anterior uveitis to panuveitis. The most common is anterior uveitis (84.7%), followed by posterior (10.2%) and intermediate (2.6%). 2)
QCan eye drops also cause uveitis?
A
Yes, uveitis has been reported with topical ophthalmic medications such as brimonidine (glaucoma eye drops) and prostaglandin analogs. In particular, brimonidine can develop from several weeks up to 5 years after initiation, and may be missed if the patient does not report using eye drops. 1)
The pathogenesis of drug-induced uveitis is broadly divided into direct mechanisms and indirect mechanisms. 1)
Direct mechanism: Direct toxicity of the drug, metabolite, or excipient disrupts the blood-ocular barrier (BAB/BRB), allowing inflammatory cells to infiltrate. Onset usually occurs within 24 to 48 hours.
Indirect mechanisms (three main pathways):
Immune complex deposition: Drug-induced antibodies form immune complexes that deposit in uveal tissue, releasing TNF-α and IL-6 (e.g., bisphosphonates)
Antigen release after microbial killing by antibiotics: Cell wall proteins of killed microbes form immune complexes (e.g., rifabutin)
Immune cell activation: Immune checkpoint inhibitors activate T cells that target uveal antigens
Drug-induced uveitis is a diagnosis of exclusion. Infectious uveitis (e.g., HSV, VZV, cytomegalovirus, toxoplasma) and autoimmune uveitis must be ruled out.
Discontinuation of the causative drug is the most important treatment.
However, in cancer immunotherapy, life-prolonging effects may outweigh the risk of uveitis.
Consultation with the prescribing physician (oncology, rheumatology, etc.) is necessary before discontinuation.
Anterior uveitis: Usually manageable with topical steroid eye drops.
Posterior uveitis/retinal vasculitis: Requires systemic steroids or local steroid injection.
If re-administration is planned, an ophthalmology visit within 1–2 weeks after administration is recommended. 1)
Treatment: Intensive topical steroids. Systemic steroids for severe cases. In mild cases, continuation of the same drug may be possible, but discontinuation or switching is often required.
A large retrospective study of 67,517 glaucoma patients compared the incidence of uveitis by topical glaucoma medication, with the following results. 2)
Drug class
Uveitis incidence
Odds ratio vs. PGA
PGA (prostaglandin analogs)
0.32%
Reference
Beta-blockers
1.95%
6 times higher
Alpha agonists
1.63%
5 times higher
Carbonic anhydrase inhibitor
1.68%
6 times higher
The common belief that PGA causes uveitis has been disproven by large-scale data.2)
Even in patients with a history of uveitis, no increase in inflammatory flares was observed with PGA.
Brimonidine eye drops: Can cause granulomatous anterior uveitis. Onset occurs from 1 week to up to 5 years after initiation.1)
Prognosis is good with discontinuation plus topical steroids, but recurrence occurs upon rechallenge.
Mepranolol (beta-blocker): The most common beta-blocker to cause uveitis. Resolves 3–5 weeks after discontinuation.
QIf I have both glaucoma and uveitis, can I use prostaglandin eye drops?
A
Large-scale studies have shown that PGAs have the lowest incidence of uveitis compared to other glaucoma medications (beta-blockers, alpha-agonists, carbonic anhydrase inhibitors), and no increased risk of recurrence was found even in patients with a history of uveitis. Avoiding PGAs due to uveitis concerns may result in missing the opportunity to receive the most effective intraocular pressure-lowering therapy. 2)
Immune checkpoint inhibitors (anti-PD-1, anti-CTLA-4, etc.): Uveitis occurs due to T cell activation. It can range from anterior to panuveitis and retinal vasculitis. Cytokine storms involving TNF-α, IL-17, and IL-2 cause tissue damage and disruption of the blood-ocular barrier. 1) The decision to continue or discontinue the drug should be made through multidisciplinary discussion, considering the life-prolonging effects of cancer therapy.
TNF inhibitors (etanercept, etc.): These often suppress uveitis in patients with arthritis, but there are also reports of inducing uveitis. For etanercept-induced uveitis, switching to adalimumab or infliximab is an option. 1)
BRAF and MEK inhibitors: Used for melanoma treatment. There is a risk of uveitis. 1)
Drug-induced tubulointerstitial nephritis and uveitis (TINU) syndrome is an independent disease entity presenting with acute interstitial nephritis + bilateral anterior uveitis.
It has been reported after use of drugs such as flurbiprofen, antibiotics (commonly used for respiratory infections: 24% of cases), and nonsteroidal anti-inflammatory drugs.
Treatment: discontinuation of the causative drug + topical steroids (systemic steroids in severe cases).
:::caution Note
Drug-induced uveitis is a diagnosis of exclusion.
In immunocompromised patients, infectious uveitis (especially CMV and tuberculosis) should be ruled out before diagnosis.
Be aware of potential reactivation of latent tuberculosis even after discontinuation of TNF inhibitors.1)
:::
The final common pathway of drug-induced uveitis is disruption of the blood-ocular barrier.
The mechanism of BRB disruption varies by drug.3)
Drug
Mechanism of action
BRB disruption mechanism
Brimonidine
Selective α2 agonist
Increased production of inflammatory cytokines
Bisphosphonates
Osteoclast function inhibition
Idiosyncratic immune reaction (T cell activation)
Brolucizumab
Anti-VEGF
Type IV hypersensitivity reaction (increase in inflammatory cytokines such as CCL2, IL-6, IL-8, ICAM-1)3)
Immune checkpoint inhibitors
Blockade of immunosuppressive receptors
Increased autoimmune reaction rate
In the case of brolucizumab, it has been confirmed that after intravitreal injection, CD4+ T cells, CD8+ T cells, CD20+ B cells, and CD68+ histiocytes accumulate in the vitreous, exacerbating inflammation. 3)
HORV is thought to be a type III hypersensitivity reaction (deposition of antigen-antibody complexes on vessel walls), but histologically, it has also been suggested that non-granulomatous choroiditis may be a primary choroidal process leading to retinal vascular necrosis. 1)
In recent years, reports of uveitis following COVID-19 mRNA vaccination have increased. Three mechanisms have been proposed: (1) direct infection from live attenuated vaccines, (2) accumulation of adjuvants/additives in uveal tissue, and (3) immune cross-reactivity with ocular structures due to molecular mimicry. 1)
Challenges in the Era of Immune Checkpoint Inhibitors
With the widespread use of novel anticancer drugs, the scope of drug-induced uveitis is expanding. Most evidence comes from case reports and retrospective studies; prospective studies and registries are needed to quantify incidence and outcomes. 1)
Collaboration among ophthalmologists, oncologists, rheumatologists, general practitioners, and pharmacists is essential for early recognition and appropriate management of drug-induced uveitis.
Pharmacists and optometrists often serve as the first point of contact, and their role in early recognition is significant. 1)
:::danger Disclaimer
This article is educational content intended to provide medical information.
For diagnosis and treatment of individual patients, please consult your primary care physician or specialist.
Please refrain from self-diagnosis or self-treatment based on the information in this article.
In particular, if you are using anticancer drugs such as immune checkpoint inhibitors, do not discontinue medication on your own without consulting your doctor, even if symptoms of uveitis appear.
:::
Lu LM, Wilkinson VMT, Niederer RL. Drug-induced uveitis: patterns, pathogenesis and clinical implications. Clin Optometry. 2025;17:141-161. doi:10.2147/OPTO.S492202
Chauhan MZ, Elhusseiny AM, Marwah S, et al. Incidence of uveitis following initiation of prostaglandin analogs versus other glaucoma medications: a study from the sight outcomes research collaborative repository. Ophthalmol Glaucoma. 2024;8(2):126-132. doi:10.1016/j.ogla.2024.10.010
Tomkins-Netzer O, Niederer R, Greenwood J, et al. Mechanisms of blood-retinal barrier disruption related to intraocular inflammation and malignancy. Prog Retin Eye Res. 2024;99:101245. doi:10.1016/j.preteyeres.2024.101245
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.