Appearance
Color tone: White to yellowish-white. Indistinct borders with a fluffy, cotton-wool-like texture.
Size: Usually less than 1/3 of the optic disc area

Cotton wool spots are small, yellowish-white (grayish-white), slightly elevated lesions that appear on the superficial retina. They are also called “soft exudates.”
It is not normal to observe cotton wool spots in a healthy patient. Even a single spot in one eye is highly likely to be the earliest fundus finding of diabetic retinopathy or hypertensive retinopathy. Among patients with cotton wool spots and no relevant history, 50% have elevated diastolic blood pressure of 90 mmHg or higher, and 20% have elevated blood glucose levels.
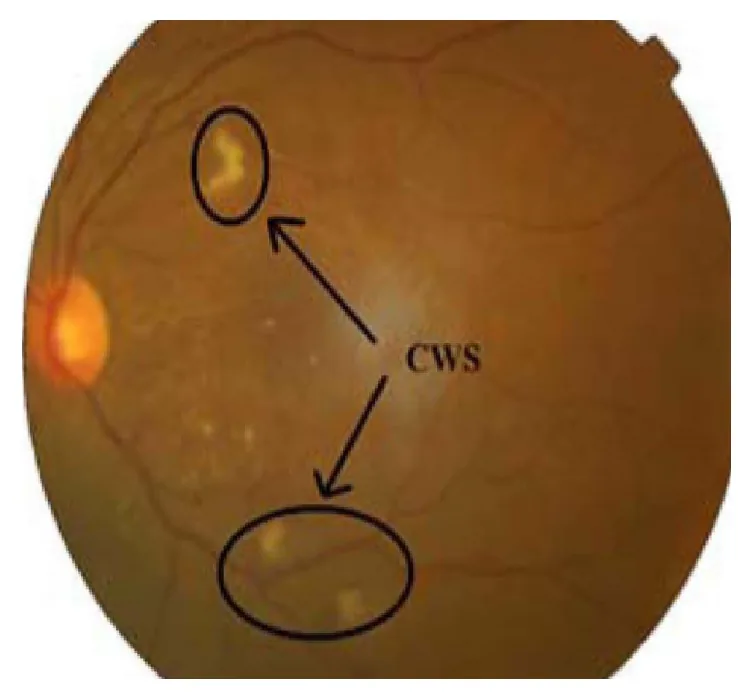
Lesions commonly occur around the optic disc and along the superior and inferior temporal arcade vessels. They are observed as ill-defined white to yellowish patchy lesions.
The lesions resolve over time. They usually disappear within 6 to 12 weeks, but may persist longer in patients with diabetic retinopathy.
Appearance
Color tone: White to yellowish-white. Indistinct borders with a fluffy, cotton-wool-like texture.
Size: Usually less than 1/3 of the optic disc area
Common Sites
Peripapillary area: May occur multiple times around the optic disc
Along the arcades: Appears along the superior and inferior temporal arcades
Course
Spontaneous resolution: Usually disappears within 6–12 weeks
Persistent cases: May persist longer in diabetic retinopathy
Clinical Significance
Not normal: An abnormal finding not seen in healthy eyes
Sign of systemic disease: An ocular sign of systemic conditions such as hypertension and diabetes
Generally, cotton wool spots themselves do not cause visual symptoms. If the fovea is involved, decreased visual acuity may occur. Systemic symptoms due to the underlying disease may also be present.
Examples of symptoms associated with each causative disease are shown below.
On dilated fundus examination, it appears as a slightly elevated, white lesion with indistinct borders on the superficial retina of the posterior pole. The lesion has a tufted margin and is characterized by a soft, cotton-wool-like texture. It is often mistaken for myelinated nerve fibers, but differs in both shape and texture.
The following table shows the differential diagnosis of major white lesions.
| Lesion Name | Color/Texture | Layer Involved |
|---|---|---|
| Soft exudates (cotton-wool spots) | White, soft, indistinct borders | Nerve fiber layer |
| Hard exudates | Yellow, hard, distinct borders | Outer plexiform layer |
| Drusen | Yellow-white, granular | Sub-retinal pigment epithelium |
Findings from representative cases are shown below.
There is no direct treatment for cotton wool spots themselves. The lesions usually resolve spontaneously within 6 to 12 weeks. The highest priority is to identify and treat the underlying disease; in suspected GCA, emergency intervention is necessary to prevent vision loss. For details, see the section on “Standard Treatment.”
Cotton-wool spots are not a specific disease but a fundus sign of various systemic and local diseases. The causes are broadly classified into four categories.
Ischemic
Hypertension: The most common cause. Also appears in renal hypertension.
Diabetes: An early finding of diabetic retinopathy.
Others: Retinal vein occlusion, ocular ischemic syndrome, anemia (red blood cell count less than 50% of normal), hyperviscosity syndrome, hypercoagulable state, radiation exposure, acute blood loss.
Immune/Inflammatory
GCA (Giant cell arteritis): 15-25 per 100,000 people over age 50. May present as bilateral cotton-wool spots3).
Collagen diseases: SLE (soft exudates prominent), dermatomyositis, scleroderma, polyarteritis nodosa.
Infectious
HIV retinopathy: various findings such as soft exudates, hemorrhages, Roth spots
Others: cat scratch disease, Rocky Mountain spotted fever, leptospirosis, bacteremia, fungemia
Other
Embolic: Purtscher-like retinopathy (carotid embolism, cardiogenic embolism, drug-induced)
Neoplastic: leukemia (venous dilation, tortuosity, hemorrhage, cotton-wool spots, Roth spots), lymphoma, metastasis
COVID-19: Cotton-wool spots were observed in 6 of 27 (22%) patients recovering from pneumonia 2)
Chemotherapeutic agents (gemcitabine, cisplatin) can cause cotton-wool spots as Purtscher-like retinopathy. Diabetes and hypertension increase the risk of gemcitabine-induced Purtscher-like retinopathy. 1)
In COVID-19, hypercoagulability and vasculitis due to direct viral infection of vascular endothelium are considered mechanisms. 2)
Retinal vein occlusion (RVO) may present with cotton-wool spots as an early clinical finding. 4)
Hypertension and diabetes are the most common causes. Even in patients without a history, 50% of those with cotton wool spots have elevated diastolic blood pressure of 90 mmHg or higher, and 20% have elevated blood sugar levels.
Diagnosis is usually made by dilated fundus examination. After confirming the lesion, it is essential to investigate the underlying disease.
The following are the main imaging tests and their findings.
| Test | Main Findings |
|---|---|
| Fundus Examination | White, poorly demarcated elevated lesion (at the level of the nerve fiber layer) |
| OCT | Focal thickening with hyperreflectivity of the nerve fiber layer (acute phase) → inner layer thinning (resolution phase) |
| FA | Adjacent capillary non-perfusion area |
Detailed findings of each examination are shown below.
Evaluation of cotton wool spots is also required in the differential diagnosis of retinal artery occlusion. 5)
The following initial tests are performed:
Additional tests that may be performed as needed are as follows:
It is important to differentiate from myelinated nerve fibers, hard exudates, retinal infiltration, retinitis, drusen, and chorioretinal atrophy.
Initial tests include blood pressure measurement, HbA1c, CBC, and HIV testing. If necessary, echocardiography, carotid ultrasound, ESR, CRP, and coagulation tests may be added. In suspected GCA, temporal artery ultrasound is useful for differential diagnosis and may require urgent management.
There is no direct treatment for cotton wool spots themselves. Identifying and treating the underlying disease is essential. The lesions usually resolve spontaneously within 6 to 12 weeks.
In HIV-infected patients with CD4 count below 200, new cotton wool spots may be an early sign of viral retinitis and require attention.
The following summarizes treatment and outcomes by underlying disease.
| Underlying disease | Treatment | Outcome |
|---|---|---|
| GCA | High-dose steroid therapy | Resolves within months3) |
| Hypertension | Antihypertensive therapy | Resolves within months |
| Anemia | Treat underlying cause | Resolves with blood improvement |
In many cases, they resolve without sequelae. However, if the fovea is involved or optic neuropathy due to GCA occurs, visual impairment may persist. In GCA, up to 20% of patients experience permanent vision loss. 3)
Cotton-wool spots occur following ischemia due to occlusion of retinal arterioles. They are associated with local accumulation of axoplasmic transport debris and are a sign of retinal ischemia. 3)
The process follows: microinfarction of retinal arterioles → occlusion of precapillary arterioles → infarction of the nerve fiber layer.
Local ischemia blocks axoplasmic flow. Mitochondria and intracellular materials accumulate within the blocked axons, causing swelling of nerve fibers. This swollen tissue appears as white to yellowish-white lesions on the fundus.
Histologically, cytoid bodies are characteristic findings. Cytoid bodies are eosinophilic fragments of swollen ganglion cell axons, filled with accumulated mitochondria and intracellular materials.
Cotton-wool spots due to specific causes follow the mechanism of Purtscher-like retinopathy.
Reports of retinal microvascular disorders in COVID-19 patients are increasing. Cotton-wool spots were observed in 6 out of 27 (22%) recovered COVID-19 pneumonia patients, drawing attention to the effects of SARS-CoV-2 on vascular endothelium. 2) Visualization of flow voids by OCT-A is contributing to disease assessment.
Tocilizumab has been shown to be effective in preventing relapse in GCA treatment. It is expected to prolong time to relapse and reduce cumulative steroid dose. 3) Temporal artery ultrasound is becoming widespread as a non-invasive diagnostic method for GCA. Reports of 100% specificity for bilateral halo sign contribute to improved diagnostic accuracy. 3)
Awareness of retinal toxicity from chemotherapeutic agents such as gemcitabine is increasing. The risk is particularly high in patients with diabetes or hypertension, and the importance of regular ophthalmic monitoring during chemotherapy is emphasized. 1)
Brummer SR, Joffe JA, Liggett PE.. Chemotherapy-Induced Retinopathy in a Diabetic and Hypertensive Patient With Stage 4 Metastatic Pancreatic Adenocarcinoma. J Vitreoretin Dis. 2023;7(3):242-244. doi:10.1177/24741264231157140. PMID:37188211; PMCID:PMC10170613.
Bottini AR, Steinmetz S, Blinder KJ, Shah GK.. Purtscher-Like Retinopathy in a Patient with COVID-19. Case Rep Ophthalmol Med. 2021;2021:6661541. doi:10.1155/2021/6661541. PMID:33859855; PMCID:PMC8009727.
Fu L, O’Sullivan EP. Giant Cell Arteritis Presenting as Bilateral Cotton Wool Spots. Cureus. 2022;14(10):e29804. doi:10.7759/cureus.29804. PMID:36337822; PMCID:PMC9620483.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal Vein Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P303-P343. doi:10.1016/j.ophtha.2024.12.025. PMID:39918523.
Kovach JL, Bailey ST, Kim SJ, Lim JI, Vemulakonda GA, Ying GS, et al. Retinal and Ophthalmic Artery Occlusions Preferred Practice Pattern®. Ophthalmology. 2025;132(4):P270-P302. doi:10.1016/j.ophtha.2024.12.024. PMID:39918522.