Post-refractive surgery ectasia (iatrogenic keratectasia / post-refractive surgery ectasia) is a condition in which the corneal stroma progressively and eccentrically thins after refractive surgery such as LASIK, PRK, or SMILE, causing steepening of the anterior and posterior surfaces. It is considered one of the most serious complications of refractive surgery and is also listed in the Refractive Surgery Guidelines (8th edition) as a postoperative complication of excimer laser surgery1).
It is irreversible and greatly reduces both uncorrected visual acuity and spectacle-corrected visual acuity. If progression is confirmed, early treatment affects the outcome.
The overall prevalence of postoperative ectasia has been reported to be 0.02–0.6%. Corneal ectasia is thought to result from insufficient corneal thickness, worsening of pre-existing subclinical keratoconus, and postoperative manifestation of genetically determined ectatic disease9). Even in cases with identified risk factors, there have been reports of ectasia developing in people with none of the known factors, and it is especially common in younger patients.
It is estimated that up to 6% of people seeking refractive surgery have some form of subclinical ectatic disease, so the accuracy of preoperative screening affects the incidence9).
The cap may contribute to corneal strength to some extent2)
The incidence after LASIK is about 4.5 times that after PRK3). However, SMILE has a short post-approval follow-up period, so it may be underestimated3).
QDoes SMILE mean you won't get ectasia?
A
SMILE is considered to have a lower ectasia rate than LASIK (11 vs 90 per 100,000 eyes)3), but the risk does not disappear. It has been suggested that the cap may contribute to corneal strength to some extent2), but the follow-up period is still short and there is concern that the long-term rate may be underestimated. In SMILE, corneal ectasia is also listed as a postoperative complication1), and preoperative screening and adherence to safety thresholds are essential.
Alvani A, Hashemi H, Pakravan M, Aghamirsalim MR. Corneal ectasia following photorefractive keratectomy: a confocal microscopic case report and literature review. Arq Bras Oftalmol. 2023;87(6):e2021-0296. Figure 2. PMCID: PMC11629660. DOI: 10.5935/0004-2749.2021-0296. License: CC BY.
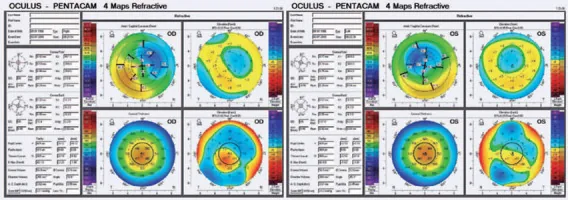
Pentacam 4 Maps Refractive in a case that developed bilateral ectasia 7 years after PRK (left: right eye OD, right: left eye OS). In both eyes, the axial curvature map shows a red-to-orange steepening pattern concentrated in the inferior temporal area, and the pachymetry map confirms inferior decentration of the thinnest point. This shows the postoperative manifestation of latent ectasia that was missed on preoperative screening. It corresponds to the postoperative manifestation of latent ectasia discussed in the “Risk Factors and Preoperative Screening” section.
The most important way to prevent ectasia is a thorough preoperative risk assessment.
In the comprehensive review of risk factors by Jin et al.7), the importance of combining corneal shape, tomography, and biomechanical assessments in predicting postoperative ectasia was emphasized, showing that a single metric is not sensitive enough. The Randleman et al.14) risk scoring system is widely used as a practical tool that improves the accuracy of preoperative screening by combining five factors.
Corneal Parameters
Keratoconus (including forme fruste): The most important factor. Clearly listed as a contraindication in the 8th edition of the guidelines1)
Insufficient RST (residual stromal bed): Risk rises sharply when RST <280μm. RST <250μm is not allowed2)
High LT index: Risk increases when the ratio of maximum ablation depth to central corneal thickness (LT/CCT) exceeds 28%2)
High PTA: A tissue alteration rate of ≥40% is significantly associated with LASIK ectasia risk4)
Evidence-based international guidelines for KLEx (small-incision corneal lenticule extraction) recommend the following safety thresholds2).
Metric
Safety criterion
Contraindication
RST (residual stromal bed)
≧280μm
<250μm (not acceptable even after accounting for measurement error)
LT index (LT/CCT ratio)
≦28%
Over 28%
PTA (percent tissue altered) *LASIK
<40%
≧40%
In SMILE (KLEx), the interpretation of PTA calculations differs from LASIK. Because the cap, unlike a flap, contributes to corneal structural strength, there is debate about applying LASIK PTA thresholds as they are2).
In the ectasia risk scoring system proposed by Randleman et al., each of the following five factors is assigned 0 to 4 points for an overall assessment14).
Corneal topography and RST alone do not achieve sensitivity above 70% for predicting postoperative ectasia2). Comprehensive evaluation using multimodal data is necessary. As biomechanical criteria suggesting ectasia, CBI (Corvis Biomechanical Index) > 0.5 and TBI (Tomographic and Biomechanical Index) > 0.29 have been proposed, and TBI (SUCRA 96.2) and CBI (SUCRA 83.8) are useful for early keratoconus detection2).
AlShawabkeh M, Al Sakka Amini R, Alni’mat A, Al Bdour MD. Unilateral Corneal Ectasia After Bilateral Transepithelial Photorefractive Keratectomy. Cureus. 2024;16:e76189. Figure 3. PMCID: PMC11749241. DOI: 10.7759/cureus.76189. License: CC BY 4.0.
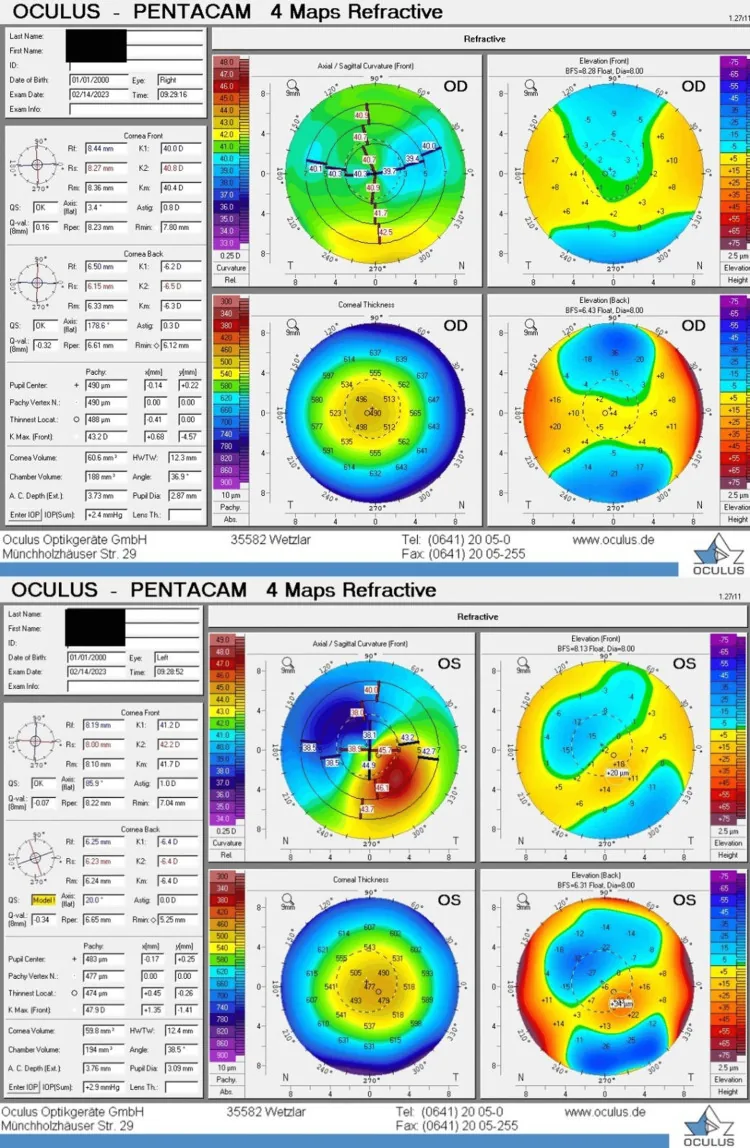
Pentacam 4 Maps Refractive of both eyes (top: right eye OD, bottom: left eye OS). In the normal right eye in the top row, both the axial curvature map and pachymetry map show a uniform distribution; in the left eye in the bottom row, a localized red-to-orange steepening inferiorly on the axial curvature map (inferior focal steepening) is seen as a typical sign of ectasia, and anterior protrusion (elevation increase) is also confirmed on the posterior elevation map. This corresponds to the inferior steepening, increased posterior elevation, and I/S asymmetry discussed in the Clinical findings and diagnosis section.
Increased discomfort with contact lenses (poor fit, frequent dislodgement)
Rapid changes in refractive error; frequent changes in glasses prescription become necessary
Distortion in the lower or nasal field of view (corresponding to the direction of the corneal protrusion)
Early symptoms are mild, and the condition is often found incidentally on corneal topography during follow-up. In particular, comparison with preoperative baseline corneal topography is essential for early detection. Serial Scheimpflug tomography (e.g., Pentacam) every 3–6 months after surgery is recommended5).
Corneal tomography (Tomography): Scheimpflug cameras (Pentacam, etc.) allow 3D evaluation of the cornea (anterior and posterior surfaces + full corneal thickness map)9). Corneal topography (Topography) images only the anterior corneal surface based on Placido disks, whereas tomography can evaluate both the anterior and posterior surfaces, so it is considered essential for early diagnosis of postoperative ectasia.
Belin-Ambrósio Enhanced Ectasia Display (BAD): Software available on Pentacam that analyzes nine parameters and calculates the “D value (BAD-D)“9). A BAD-D > 1.65 is the threshold for suspected ectasia and is useful as a multivariable index integrating anterior elevation, posterior elevation, and pachymetric data.
Epithelial thickness mapping: The “doughnut pattern” of central epithelial thinning and surrounding epithelial thickening is characteristically seen in corneal ectasia9). It is assessed with high-resolution AS-OCT or high-frequency ultrasound.
Wavefront aberration analysis: Useful for confirming increased higher-order aberrations (with coma predominance).
Anterior segment OCT (AS-OCT): Allows full-thickness corneal cross-sections, flap-depth confirmation, and pachymetry mapping.
In the 2015 international consensus, “progression of ectasia” was defined as consistent changes exceeding measurement noise in at least two of the following parameters5).
Reports indicate that 77% of younger patients (18 years or younger) showed tomographic progression10), and serial evaluation every 3 to 6 months with the same device is recommended.
Postoperative ectasia and naturally occurring keratoconus have similar corneal shapes and clinical findings, but whether there is a history of refractive surgery is the key to telling them apart. Cases in which suspected keratoconus was treated and ectasia became apparent after surgery, and postoperative ectasia in a normal cornea, are also pathophysiologically continuous in some respects6). When making the differential diagnosis, it is important to check the surgical record (flap thickness, ablation depth, postoperative RST).
QHow is ectasia different from keratoconus?
A
Corneal ectasia is an iatrogenic condition after refractive surgery, whereas keratoconus is a naturally occurring degenerative disease. However, the clinical features of both (corneal thinning, steepening, and irregular astigmatism) and the mechanism of onset (breakdown of corneal biomechanics) are essentially similar, and many cases are thought to involve latent keratoconus becoming apparent after surgical stress6). The basic approach to differentiation is to confirm whether there was a prior surgery and to review preoperative data.
QWhat tests are needed to assess the risk of ectasia?
A
Corneal shape analysis with a Placido disk alone is not enough. A three-dimensional assessment of the anterior and posterior surfaces and corneal thickness using Scheimpflug tomography (Pentacam, etc.) is essential. A comprehensive evaluation combining calculation of the BAD-D value, epithelial thickness mapping with AS-OCT, and corneal biomechanics measurements (Corvis ST, etc.) is recommended2).
The treatment strategy for ectasia has two main goals: 1) preventing progression and 2) correcting and restoring visual function. Early intervention once progression is confirmed is important for preserving vision.
It is the first-line treatment for confirmed progressive ectasia1)9). The aim of CXL is to stabilize the corneal structure by strengthening cross-links between corneal collagen, and the following protocols are used.
Standard method (Dresden protocol): After removing the corneal epithelium within an 8–9 mm diameter, 0.1% riboflavin eye drops are instilled for 30 minutes (every 2 minutes), followed by ultraviolet A (UVA: 370 nm, 3 mW/cm²) irradiation for 30 minutes. The total UVA energy is 5.4 J/cm². A long-term stabilizing effect has been established9).
Accelerated method (accelerated CXL): Higher-intensity UVA is delivered for a shorter time (e.g., 9 mW/cm² × 10 min, 30 mW/cm² × 3 min). Treatment time can be shortened, but some reports indicate that long-term outcomes are inferior to the standard method, and optimization of energy density is being studied11).
Transepithelial CXL: A protocol in which riboflavin is allowed to penetrate without removing the epithelium. Although less invasive, many reports show that the effect is inferior to the standard method9).
After CXL, progression stops in many cases, and a slight improvement in corneal steepness (flattening by about 1.0–2.5 D) may also be seen9). The U.S. FDA has approved CXL for progressive keratoconus and post-refractive surgery ectasia in patients aged 14 to 65, and in Japan it has been covered by insurance since 2022.
In a U.S. multicenter trial by Hersh et al.15), CXL for post-refractive surgery ectasia met efficacy and safety criteria, and a significant decrease in maximum corneal curvature (Kmax) and stabilization of corneal shape were confirmed 1 year after treatment. Compared with the untreated control group, progression was significantly suppressed in the treatment group, demonstrating the effectiveness of early CXL intervention for ectasia15).
Contraindications for CXL: A corneal stromal thickness of less than 400 μm during UVA irradiation is contraindicated because of the risk of endothelial damage9).
Complications of CXL: punctate keratitis, corneal haze, photophobia, pain, infectious keratitis, sterile infiltrates, nonhealing epithelial defects, corneal edema, and others9).
Early CXL in young patients: In young patients (prepubertal and adolescents), early CXL intervention is recommended without waiting for symptoms to worsen9). The KERALINK trial showed that CXL is effective in progressive keratoconus in patients 18 years and younger, and a systematic review supports that CXL can reduce the need for corneal transplantation over the long term12).
These are a mainstay for vision correction when irregular corneal astigmatism reduces corrected visual acuity. They correct irregular astigmatism optically by forming a tear lens behind the lens. They are effective in mild to moderate ectasia and allow many patients to maintain daily visual function. Scleral lenses are effective in advanced cases and irregular corneas. Good centering and movement are important for fitting, and if spherical lenses are not suitable, lenses with multiple curves can also be chosen9).
This approach simultaneously reduces irregular corneal astigmatism and stabilizes the corneal structure in advanced ectasia. Planning methods such as the Athens protocol (Kanellopoulos) and the LYRA/San Diego protocol (Motwani) have been reported11). RSB > 350 μm, a maximum ablation depth within 50–60 μm, and same-session CXL are recommended, but the evidence is still limited.
Treatment with the LYRA/San Diego protocol has been reported to improve uncorrected visual acuity to 20/20 and significantly reduce higher-order aberration (HOA) RMS (from 1.642 to 0.920)11); when combined with corneal strengthening through simultaneous CXL, it is expected to provide greater long-term stability than topography-guided PRK alone. However, this procedure is performed only at specialized centers and requires a comprehensive preoperative evaluation and full informed consent from the patient.
ICRS involves implanting PMMA or polycarbonate semicircular implants within the corneal stroma to mechanically support the peripheral cornea and reduce irregular astigmatism in the central cornea9). Several designs, such as the Ferrara ring and Intacs, are available, and choosing the placement and thickness according to the corneal shape is important. Femtosecond laser channel creation is now the standard method and is more precise than the mechanical approach. ICRS is intended to improve visual function (better UCVA and BCVA, and reduced higher-order aberrations) and can also help improve contact lens fitting. In some cases, a combined approach with CXL (usually CXL first or CXL 1 to 6 months after ICRS) may be recommended9).
This is considered in advanced cases with corneal clouding or scarring when correction with contact lenses is not possible. Penetrating keratoplasty (PKP) has traditionally been the standard, but when endothelial function is normal, deep anterior lamellar keratoplasty (DALK) is an option. DALK carries no risk of endothelial rejection and may cause less long-term endothelial cell loss than PKP9).
QCan ectasia be cured?
A
Current treatment cannot achieve cure (restoration to the original corneal shape), but corneal cross-linking (CXL) can stop progression. After CXL, the corneal shape stabilizes in many cases, and vision correction with contact lenses or glasses can continue. In advanced cases, combining CXL with topography-guided PRK or intracorneal ring segments (ICRS) may improve irregular astigmatism. As a last resort, corneal transplantation may restore visual function.
5. IOL power calculation when cataract surgery is combined
As ectasia progresses, it causes myopia and irregular astigmatism, and if cataract is also present, calculating intraocular lens (IOL) power becomes extremely difficult. When standard IOL formulas are used, postoperative hyperopic surprise is likely, so specialized management is needed13).
Overestimation of refractive power due to steepening of the posterior cornea: standard corneal measurements use a fixed conversion factor (n=1.3375), but in ectasia the anterior-to-posterior surface ratio changes, causing overestimation
Measurement uncertainty due to irregular astigmatism: asymmetry of the axial curvature map makes it difficult to choose a representative corneal curvature value
Overlap of surgical effects: prior refractive surgery (corneal shape changes) and ectasia overlap, and standard formulas do not correct enough
ELP (effective lens position) prediction error: the abnormal combination of corneal shape and anterior chamber depth makes ELP prediction difficult
IOL power calculation using TK (True Keratometry) values obtained by Scheimpflug tomography such as Pentacam (using direct measurements of the anterior and posterior surfaces)13)
Use of formulas designed for post-refractive surgery eyes, such as Abulafia-Koch, Barrett True K (post-LASIK), and Potvin-Hill Pentacam
After corneal transplantation, consider special calculations using the retroreflection method (Haigis-L, etc.) or eccentric measurements
Set the preoperative target refraction toward emmetropia to mild myopia (a conservative approach) to avoid a hyperopic surprise
Explain the uncertainty of IOL power calculation to the patient in sufficient detail, and if needed, plan postoperative refractive correction (glasses or contact lenses) in advance
6. Pathophysiology and detailed mechanisms of onset
The essence of ectasia after refractive surgery is failure of corneal biomechanics caused by surgical invasion. Damaging the lamellar structure of the anterior stroma (the strong collagen just beneath Bowman’s membrane) reduces the cornea’s resistance to intraocular pressure. Creating a LASIK flap completely frees the anterior stroma, so it is considered biomechanically less favorable than the cap design of SMILE. In the mathematical model by Reinstein et al., the relative corneal tensile strength of PRK, LASIK, and SMILE was quantified, and compared with LASIK, SMILE preserves the anterior stroma and therefore maintains more corneal strength for the same amount of correction8).
Disruption of corneal biomechanics progresses step by step. Immediately after surgery, the cornea becomes easier to deform even within the normal range of intraocular pressure (biomechanical vulnerability), and latent corneal deformation may become apparent over several months to several years after surgery. This process can be promoted by secondary insults such as the habit of rubbing the eyes, chronic mechanical irritation from allergies, or additional corrective surgery (enhancement). As indices for evaluating biomechanics, CH (corneal hysteresis) and CRF (corneal resistance factor) can be monitored from before surgery through after surgery to capture changes in progression risk. If these values continue to decrease after surgery, this may be interpreted as a sign of impending ectasia. Regular postoperative biomechanical measurements such as Corvis ST can help with early detection of ectasia9).
In many cases, a fine weakness in corneal biomechanics that could not be detected before surgery (latent or subclinical keratoconus) becomes apparent after surgical stress. The first report of ectasia after LASIK in forme fruste keratoconus was published in 19986).
Forward shift in posterior corneal elevation is recognized as an early sign of ectasia. In some cases, the posterior surface changes before the anterior surface, so tomography that includes posterior surface assessment is essential for early diagnosis.
The causes of corneal ectasia involve abnormal enzyme activity and oxidative stress9). In the cornea, increases in matrix metalloproteinases (MMPs) and decreases in TIMPs (tissue inhibitors of metalloproteinases) are observed, and breakdown of the extracellular matrix progresses. In patients with genetic predisposition, including collagen disorders such as Ehlers-Danlos syndrome and osteogenesis imperfecta, ectasia is more likely to become apparent when environmental secondary triggers such as eye rubbing or iatrogenic thinning from surgery are added9).
Comprehensive evaluation of postoperative ectasia risk factors
A review by Jin et al.7) identified abnormal corneal shape, thin corneas, insufficient RST, high myopia, young age, and the habit of rubbing the eyes as major risk factors for postoperative ectasia, and showed that a combined risk score is useful for preoperative decision-making. In the scoring system by Randleman et al.14), abnormal corneal shape is the most important predictor, and the other factors play a supporting role. In a study by Shetty et al.16), biomechanical changes after SMILE and LASIK were compared, showing that SMILE preserved better corneal strength indices (CRF and CH) at 12 months after surgery. This advantage is thought to contribute to differences in the incidence of postoperative ectasia16).
In a 2-year outcome study of accelerated CXL (9 mW/cm²×10 min) for LASIK-related ectasia, progression was halted in many cases and safety was confirmed11). However, with ultra-accelerated treatment (45 mW/cm²), there are concerns about thermal effects, and optimization studies using pulsed-light CXL are underway.
In the 2021 KERALINK trial12), patients aged 16 to 25 years with progressive keratoconus were compared between CXL and observation, and the CXL group showed a significant reduction in Kmax (−1.35 D) and stabilization at 3 years. These results support active use of CXL in young patients, and the same principle applies to postoperative ectasia.
Before CXL, a corneal stromal thickness of at least 400 μm is considered necessary, but for thin corneas (300–400 μm), CXL may still be possible by using hypotonic riboflavin or a sub400 protocol (expanding the cornea with a small amount of riboflavin before irradiation)9).
CXL performed at the same time as refractive surgery (LASIK-CXL) is being studied in high-risk patients (thin corneas, young age, high myopia), and is already being done at some centers. However, it is not a standard treatment at present, and more evidence from RCTs is needed.
Research is under way on new collagen cross-linking materials (for example, glucose-containing riboflavin and lutein-containing formulations) and corneal reinforcement materials using nanoparticles. There is also growing interest in using lenticules removed by SMILE as corneal inlays for keratoconus and post-surgical ectasia. This “lenticule reimplantation” approach is promising for the future because it uses autologous or allogeneic tissue without relying on corneal bank resources, but it is still at the research stage and has not yet reached routine clinical use9).
A CXL effect assessment system using the ABCD classification on Pentacam and similar devices is becoming more common. In this system, A is anterior radius curvature, B is posterior radius curvature, C is minimum corneal thickness, and D is best corrected visual acuity. It is expected to be useful as a quantitative indicator of progression. As a criterion for judging progression, the ABCD classification is highly sensitive in longitudinal comparisons using the same device, and it is also useful for comparing changes before and after CXL in the management of postoperative ectasia9).
Wang Y, Xie L, Yao K, Sekundo W, Alió JL, Mehta JS, Goel S, Elmassry A, Schallhorn J, Shilova T, Cao H, Xu L, Chen X, Zhang F, Bai J, Zhang W, Liu Q, Zhou X, Chen Y, Wang Z, Jhanji V, Yang K, Writing Committee for the Guideline Working Group. Evidence-Based Guidelines for Keratorefractive Lenticule Extraction Surgery. Ophthalmology. 2025;132(4):397-419. doi:10.1016/j.ophtha.2024.11.016. PMID:39577672.
Moshirfar M, Tukan AN, Bundogji N, Liu HY, McCabe SE, Ronquillo YC, et al. Ectasia After Corneal Refractive Surgery: A Systematic Review. Ophthalmology and therapy. 2021;10(4):753-776. doi:10.1007/s40123-021-00383-w. PMID:34417707; PMCID:PMC8589911.
Santhiago MR, Smadja D, Gomes BF, et al. Association between the percent tissue altered and post-LASIK ectasia in eyes with normal preoperative topography. Am J Ophthalmol. 2014;158:87-95.e1. doi:10.1016/j.ajo.2014.04.002. PMID:24727263.
Gomes JA, Tan D, Rapuano CJ, Belin MW, Ambrósio R, Guell JL, Malecaze F, Nishida K, Sangwan VS, Group of Panelists for the Global Delphi Panel of Keratoconus and Ectatic Diseases. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359-369. doi:10.1097/ico.0000000000000408. PMID:25738235.
Theo Seiler, Andreas W. Quurke. Iatrogenic keratectasia after LASIK in a case of forme fruste keratoconus. Journal of Cataract and Refractive Surgery. 1998;24(7):1007-1009. doi:10.1016/s0886-3350(98)80057-6.
Jin SX, Dackowski E, Chuck RS. Risk factors for postlaser refractive surgery corneal ectasia. Current opinion in ophthalmology. 2020;31(4):288-292. doi:10.1097/ICU.0000000000000662. PMID:32398416.
Reinstein DZ, Archer TJ, Randleman JB. Mathematical model to compare the relative tensile strength of the cornea after PRK, LASIK, and small incision lenticule extraction. J Refract Surg. 2013;29:454-460. doi:10.3928/1081597X-20130617-03. PMID:23820227.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Gore DM, et al. Tomographic progression of keratoconus in children and young adults. Br J Ophthalmol. 2024;108:176-182.
Manoj Motwani, Emmanuel Agu, Albert Xu, Madeline Yung. Application of Surgical Protocols for the Treatment of Highly Irregular Astigmatism with Topographic Guided Ablation in a Case of Post-LASIK Ectasia. IMCRJ. 2025;Volume 18:91-98. doi:10.2147/imcrj.s476407.
Larkin DFP, Chowdhury K, Burr JM, et al. Effect of corneal cross-linking versus standard care on keratoconus progression in young patients: The Keralink randomized controlled trial. Ophthalmology. 2021;128:1516-1526. doi:10.1016/j.ophtha.2021.04.019. PMID:33892046.
European Society of Cataract and Refractive Surgeons (ESCRS). ESCRS Clinical Guidelines for Cataract Surgery. ESCRS; 2024.
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008 Jan;115(1):37-50.e4. doi:10.1016/j.ophtha.2007.03.073. PMID:17624434.
Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK, U.S. Crosslinking Study Group. U.S. Multicenter Clinical Trial of Corneal Collagen Crosslinking for Treatment of Corneal Ectasia after Refractive Surgery. Ophthalmology. 2017;124(10):1475-1484. doi:10.1016/j.ophtha.2017.05.036. PMID:28655538.
Shetty R, Francis M, Shroff R, Pahuja N, Khamar P, Girrish M, et al. Corneal Biomechanical Changes and Tissue Remodeling After SMILE and LASIK. Investigative ophthalmology & visual science. 2017;58(13):5703-5712. doi:10.1167/iovs.17-22864. PMID:29101408.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.