
Myelinated Retinal Nerve Fibers
Key points at a glance
Section titled “Key points at a glance”1. What are myelinated retinal nerve fibers?
Section titled “1. What are myelinated retinal nerve fibers?”Myelinated retinal nerve fibers are a congenital anomaly in which focal myelination occurs in the retinal nerve fibers, which are normally unmyelinated. They were first reported by von Jager in 1855. The prevalence is approximately 0.3-1%.
Normal myelination and development of this condition
Section titled “Normal myelination and development of this condition”Normally, optic nerve fibers undergo myelination by oligodendrocytes only posterior to the lamina cribrosa. The nerve fibers anterior to the lamina cribrosa, i.e., from the optic disc into the retina, remain unmyelinated.
Normal myelination begins around the fifth month of gestation, starting from the lateral geniculate body toward the optic nerve, and stops upon reaching the lamina cribrosa. The lamina cribrosa acts as a physical barrier preventing oligodendrocytes from entering the retina.
This condition occurs when oligodendrocytes cross the lamina cribrosa and enter the retina, causing focal myelination of nerve fibers. Theories regarding the cause include structural abnormalities of the lamina cribrosa or a timing mismatch in development, but details remain unclear.
Classification
Section titled “Classification”They are morphologically classified into three types.
| Classification | Frequency | Fundus findings | Symptoms |
|---|---|---|---|
| Localized (continuous with optic disc) | Most common | White opacity spreading in a fan shape from the optic disc | Usually asymptomatic |
| Isolated | Rare | White opacity away from the optic disc | Usually asymptomatic |
| Extensive type | Rare | Extensive white opacity | Visual impairment and visual field defects |
Most cases are localized and asymptomatic, so treatment is not required. For extensive types complicated by amblyopia, occlusion therapy may be attempted, but the effect is limited. It is important to regularly follow up with an ophthalmologist to check for complications such as high myopia, amblyopia, and retinal vascular abnormalities.
2. Main symptoms and clinical findings
Section titled “2. Main symptoms and clinical findings”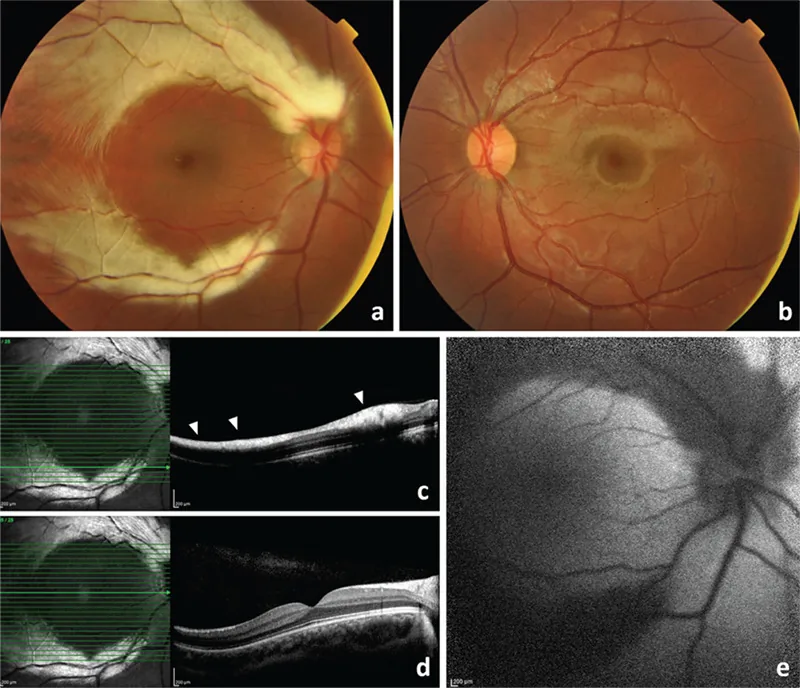
Subjective symptoms
Section titled “Subjective symptoms”Most cases are asymptomatic because the lesion is localized and small. It is often discovered incidentally during fundus examination. In the extensive type, it can cause visual impairment and visual field defects.
Fundus Findings
Section titled “Fundus Findings”The characteristic finding is a feathered edge white opacity along the course of the retinal nerve fibers. The margins are irregular and feathery, matching the direction of the nerve fiber bundles.
- Juxtapapillary type (most common): White opacity spreading in a fan shape from the optic disc, following the radial nerve fibers centered on the disc.
- Isolated type: A solitary opacity away from the optic disc, with feathery borders.
- Extensive type: Widespread white opacity affecting vision and visual field.
Various Imaging Findings
Section titled “Various Imaging Findings”- Infrared fundus photography / Red-free fundus photography: The myelin sheath contains a large amount of lipid, so it is recognized as white.
- Fundus autofluorescence (FAF): Normal autofluorescence is blocked, resulting in hypofluorescence.
- Fluorescein angiography (FA): Blocks background fluorescence, and no leakage into the lesion is observed (unlike soft drusen, there is no leakage).
- OCT: The thickness of the retinal nerve fiber layer (RNFL) shows abnormally high values corresponding to the myelinated area.
Associated Findings
Section titled “Associated Findings”In the extensive type, the following associated findings may be observed.
- High myopia: May be accompanied by elongation of the axial length
- Amblyopia: Occurs through a mechanism similar to form deprivation amblyopia, as light blockage by the myelin sheath restricts visual input during the developmental period
- Retinal vascular abnormalities: May involve abnormal or irregular course of arteries and veins
Straatsma syndrome
Section titled “Straatsma syndrome”The triad of myelinated nerve fibers, high myopia, and amblyopia is called Straatsma syndrome (or extensive myelinated nerve fiber syndrome). This concept is recognized in the extensive type and has a significant impact on visual function. It is a rare condition.
In children with extensive myelinated nerve fibers, early detection and management of amblyopia are important issues. However, the effect of amblyopia treatment is limited, and the final visual prognosis is often poor. High myopia is managed with refractive correction, but if axial myopia progresses, careful follow-up is needed with attention to the risk of myopic complications.
3. Causes and Risk Factors
Section titled “3. Causes and Risk Factors”Classification as a Congenital Abnormality
Section titled “Classification as a Congenital Abnormality”Myelinated retinal nerve fibers are a congenital developmental anomaly and are not caused by acquired factors. No specific risk factors are known. Although familial cases have been reported sporadically, heredity is rare and the mode of inheritance has not been established.
Rarely, associations with hereditary syndromes (such as GAPO syndrome, Albright hereditary osteodystrophy, and neurofibromatosis type 1) have been reported, but most cases are sporadic without associated syndromes. Acquired myelinated nerve fibers are extremely rare and have been reported in association with blunt trauma, optic disc drusen, and after optic neuritis.
Mechanism of Development
Section titled “Mechanism of Development”Myelination of the optic nerve, which begins at the lateral geniculate body around the fifth month of gestation, extends into the retina without stopping at the lamina cribrosa. This is thought to occur when the physical barrier function of the lamina cribrosa is impaired for some reason, or when the onset of myelination is early.
The effect of myelination on visual function is impaired light transmission due to the white opacity of the myelin sheath. The myelin sheath obstructs light transmission and forms a relative scotoma. In extensive cases, it can cause decreased visual acuity and visual field defects. The mechanism of amblyopia is considered similar to form deprivation amblyopia, where light blockage by the myelin sheath limits visual input during the developmental period.
4. Diagnosis and Examination Methods
Section titled “4. Diagnosis and Examination Methods”Clinical Diagnosis
Section titled “Clinical Diagnosis”Diagnosis is made based on characteristic fundus findings. Brush-like white opacities along the course of nerve fibers are typical, and the feathery edge is an important point for differentiation. Additional tests are rarely required for diagnosis, but in extensive cases, imaging and visual field tests are performed to rule out differential diagnoses.
Differential Diagnosis
Section titled “Differential Diagnosis”| Findings | Myelinated retinal nerve fibers | Soft exudates |
|---|---|---|
| Reflection | Strong (brush-like, glossy) | Weak (cotton-wool) |
| Edema | None (flat) | Present (elevated) |
| Relationship with retinal vessels | Large vessels are covered | Not covered |
| FA findings | Background fluorescence block only, no leakage | Ischemic changes with leakage |
| Location | Corresponds to nerve fiber layer | Around blood vessels |
Other diseases requiring differential diagnosis in pediatric white fundus lesions include retinoblastoma (mass-like, elevated, with calcification) and astrocytoma (white retinal nodules associated with tuberous sclerosis).
Examination
Section titled “Examination”- Fundus examination (direct/indirect ophthalmoscopy): confirmation of characteristic white opacities
- Fluorescein angiography: check for fluorescein leakage (differential diagnosis from soft exudates)
- Autofluorescence imaging: confirmation of hypoautofluorescent pattern
- Infrared imaging/red-free imaging: contrast evaluation of white opacities
- OCT: Confirmation of abnormally high RNFL thickness (corresponding to the medullated area)
- Visual field test: Indicated for extensive type. Evaluation of corresponding scotoma.
Differential diagnosis includes soft exudates (fluorescein leakage not along nerve fiber layer), retinoblastoma (children, mass, calcification), and astrocytoma (white retinal nodule associated with tuberous sclerosis). The key distinguishing feature of medullated nerve fibers is that they are strongly reflective and flat, and do not show fluorescein leakage on fluorescein angiography.
5. Standard Treatment
Section titled “5. Standard Treatment”Principle: No treatment required
Section titled “Principle: No treatment required”Most cases are localized and asymptomatic, so treatment is not required. Observation alone is sufficient, and regular ophthalmologic examinations confirm the absence of complications. It is also an important clinical measure to fully explain to patients and guardians that this is a non-progressive congenital anomaly, avoiding unnecessary anxiety.
Follow-up Guidelines
Section titled “Follow-up Guidelines”Regular fundus examinations document changes in the lesion. Usually, no enlargement in size or extent is observed, but if the lesion shrinks or disappears compared to previous records, the possibility of optic nerve damage should be considered and further examination performed. In children, visual acuity measurement and refraction testing should be performed regularly to assess the risk of amblyopia.
Management of Complications
Section titled “Management of Complications”- Amblyopia: Amblyopia treatment such as occlusion therapy (patching the healthy eye) may be attempted. However, it is considered to have little effect, and careful judgment is required before initiating treatment.
- High myopia: Appropriate refractive correction (glasses or contact lenses) should be provided. Contact lenses may be advantageous when anisometropia is severe.
- Retinal vascular abnormalities: Management according to the type of vascular abnormality. Laser photocoagulation may be performed if neovascularization or vitreous hemorrhage is present.
- Strabismus: Manage associated strabismus according to standard protocols.
6. Pathophysiology and detailed pathogenesis
Section titled “6. Pathophysiology and detailed pathogenesis”Normal process of optic nerve myelination
Section titled “Normal process of optic nerve myelination”Normal myelination of the optic nerve begins around the fifth month of gestation at the lateral geniculate body. Myelination proceeds in order through the lateral geniculate body, optic radiation, optic chiasm, optic nerve, and lamina cribrosa, where it stops. Because the lamina cribrosa acts as a physical barrier preventing oligodendrocytes from entering the retina, retinal nerve fibers normally remain unmyelinated.
Mechanism of this disease
Section titled “Mechanism of this disease”This disease occurs when oligodendrocytes cross the lamina cribrosa and enter the retina, causing focal myelination of retinal nerve fibers. The cause of this focal invasion is unknown, and the following theories have been proposed.
- Lamina cribrosa structural abnormality theory: Partial defects or structural abnormalities in the lamina cribrosa allow oligodendrocyte invasion.
- Timing mismatch theory: Myelination begins earlier than normal, allowing oligodendrocytes to enter the retina before the lamina cribrosa is formed.
Impact on visual function
Section titled “Impact on visual function”Myelin is white and opaque, obstructing light transmission. Localized myelinated nerve fibers form small relative scotomas, but due to brain plasticity, subjective symptoms are often minimal. In extensive types, they cause decreased visual acuity and visual field defects. Amblyopia is thought to arise through a mechanism similar to form deprivation amblyopia, where myelination during the developmental period impedes light transmission, limiting visual input. The poor response to amblyopia treatment suggests a significant degree of this form deprivation.
OCT Considerations
Section titled “OCT Considerations”In OCT evaluation, the RNFL thickness at the myelinated site is abnormally increased, which can lead to overestimation of RNFL thickness (segmentation error) in glaucoma diagnosis. In eyes with myelinated nerve fibers, true RNFL thinning due to glaucoma may be masked, requiring particular caution in interpreting OCT results. Comprehensive judgment should be made in conjunction with other examination findings such as visual field testing and intraocular pressure measurement.
Prognosis and Course
Section titled “Prognosis and Course”This condition is a non-progressive congenital anomaly, and the extent of myelination typically does not increase over time. In localized, isolated cases, the impact on visual function is minimal, and long-term prognosis is good. In extensive types, decreased visual acuity, visual field defects, and amblyopia persist, and the effect of amblyopia treatment is poor, leaving residual impact on visual function. Long-term follow-up is necessary when high myopia is present.
7. Latest Research and Future Prospects
Section titled “7. Latest Research and Future Prospects”Quantitative evaluation of myelinated retinal nerve fibers using OCT is advancing. An abnormally high RNFL thickness pattern has been reported (a pediatric cohort study reported that the mean RNFL thickness at the myelinated site is significantly thickened, approximately 152 μm compared to about 114 μm in the healthy eye), and its usefulness as a diagnostic aid is being investigated. Additionally, in glaucoma diagnosis, OCT evaluation may overestimate RNFL thickness, and caution is needed when interpreting eyes with myelinated nerve fibers.
There have been case reports of myelinated nerve fibers regressing after multiple sclerosis or optic neuritis. The fact that congenital myelinated nerve fibers can disappear due to inflammation or demyelinating diseases is an important finding for deepening our understanding of the natural course of this condition.
Quantitative research on the epidemiology and mechanisms of Straatsma syndrome is limited, and further accumulation of multicenter data is needed. Long-term follow-up studies have shown poor responsiveness to amblyopia treatment, while some cases have reported partial visual improvement through a combination of anisometropic correction and active occlusion therapy, leading to ongoing debate about the significance of early intervention. Many aspects of the genetic background remain unclear at present.
It is a congenital anomaly and is usually non-progressive. Basically, the size or extent does not enlarge. However, there have been case reports of myelinated nerve fibers disappearing (regressing) after multiple sclerosis or optic neuritis. Re-evaluation is also underway as to whether congenital myelinated nerve fibers are truly stable.
References
Section titled “References”-
Tarabishy AB, Alexandrou TJ, Traboulsi EI. Syndrome of myelinated retinal nerve fibers, myopia, and amblyopia: a review. Surv Ophthalmol. 2007 Nov-Dec;52(6):588-96. PMID: 18029268
-
Kee C, Hwang JM. Visual prognosis of amblyopia associated with myelinated retinal nerve fibers. Am J Ophthalmol. 2005 Feb;139(2):259-65. PMID: 15733986
-
Shen Y, Zhao J, Sun L, Zeng L, Chen Z, Tian M, Zhou X. The long-term observation in Chinese children with monocular myelinated retinal nerve fibers, myopia and amblyopia. Transl Pediatr. 2021 Apr;10(4):860-869. PMID: 34012835
-
Kera J, Fasiuddin AF. Ocular Findings Associated With Myelinated Retinal Nerve Fibers. Cureus. 2021 Apr 19;13(4):e14552. PMID: 34017666 / PMCID: PMC8130640
-
Sevik MO, Aykut A, Karaman NF, Şahin Ö. Straatsma Syndrome: Should Visual Prognostic Factors Be Taken into Account? A Case Report. Turk J Ophthalmol. 2021 Dec 28;51(6):398-402. PMID: 34963270 / PMCID: PMC8715659