Preservative toxicity in eye drops refers to the toxicity caused by preservatives in eye drops, mainly benzalkonium chloride (BAK), on the corneal and conjunctival epithelium. It is clinically important in patients who use multiple eye drops long term, especially those using several glaucoma medications.
About 70% of commercially available eye drops contain BAK. Because patients with glaucoma often need long-term use of multiple eye drops, ocular surface disease (OSD) is common. It is said that about 50–60% of patients with glaucoma have OSD10), and more than about 60% of patients using three or more BAK-containing eye drops show SPK2). Long-term BAK use has also been reported to affect postoperative outcomes after glaucoma filtering surgery5).
There are several preservatives used in eye drops, and their toxicity differs.
Preservative
Features
Typical products
BAK (benzalkonium chloride)
Most commonly used. Concentration-dependent epithelial toxicity
Many glaucoma and antibacterial eye drops
Polyquad®
Less toxic than BAK
Travatan®
SoftZIA® (zinc-based preservation system)
Low toxicity. Next-generation preservative system
Some glaucoma eye drops
Preservative-free (PF)
Safest. Unit-dose forms, etc.
Mucosta UD®,Tapros® PF
QWhy are preservatives needed in eye drops?
A
Preservatives are needed to prevent microbial contamination of eye drops after opening. Without preservatives, bacteria and fungi can grow within a few days after opening and raise the risk of infectious eye disease. However, because preservatives themselves are toxic to the ocular surface, balancing the risks and benefits is important during long-term use.
2. Symptoms and clinical findings of eye damage caused by preservatives
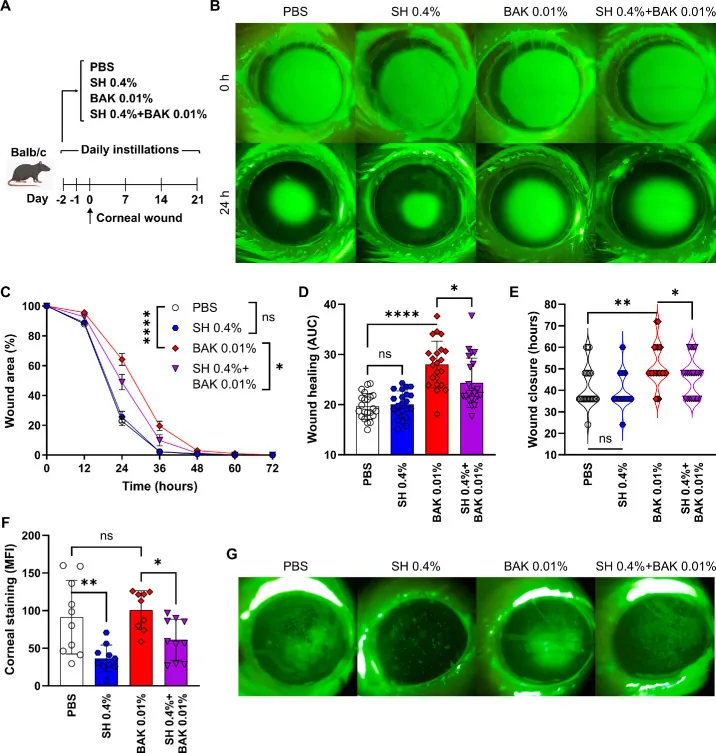
Vereertbrugghen A, Pizzano M, Sabbione F, et al. Hyaluronate Protects From Benzalkonium Chloride-Induced Ocular Surface Toxicity. Transl Vis Sci Technol. 2024;13(10):31. Figure 4. PMID: 39432403; PMCID: PMC11498636; DOI: 10.1167/tvst.13.10.31. License: CC BY 4.0.
Corneal images under fluorescein staining: the PBS control eye (top) shows almost no staining, whereas the BAK 0.01% treated eye (bottom) shows strong green fluorescent staining across the cornea, indicating marked impairment of the epithelial barrier. This corresponds to the fluorescein staining findings of BAK-induced toxic corneal epitheliopathy discussed in the section “Symptoms and clinical findings of eye damage caused by preservatives.”
Fluorescein staining: Positive punctate staining mainly in the lower cornea is a characteristic finding of BAK toxicity.
Distribution: A distribution mainly in the lower cornea, consistent with a flow pattern from the inferior fornix.
Goblet cell damage
Decreased goblet cell density: Can be quantitatively evaluated by conjunctival impression cytology.
Functional impact: Secretion of mucins such as MUC5AC decreases, shortening tear film stability (BUT).
Conjunctival changes
Conjunctival redness and papillary response: Mainly in the inferior fornix. Inflammatory changes caused by chronic irritation.
Fibrosis: Long-term, chronic exposure to BAK can cause scarring of the subconjunctival tissue.
Other findings
Delayed corneal epithelial healing: Barrier function decreases due to disruption of epithelial tight junctions.
Worsening of MGD: Because of BAK’s surfactant effect, the tear film lipid layer becomes unstable, and meibomian gland dysfunction (MGD) worsens.
QCould the stinging when I put in eye drops be due to the preservative?
A
It is possible. Eye drops containing BAK can cause a stinging or burning sensation right after instillation. If the irritation is only temporary, it is usually less concerning, but if there is persistent stinging, dryness, or a gritty feeling, it is advisable to ask an eye doctor about switching to a preservative-free formulation.
BAK is a cationic surfactant and exerts toxicity on the ocular surface through the following mechanisms1).
Cell membrane damage: It disrupts the phospholipid bilayer of corneal epithelial cells, causing cell injury. Toxicity is concentration-dependent; at 0.005% or lower, toxicity is low, but at 0.02% clear epithelial damage occurs6)
Induction of apoptosis: It activates the caspase pathway in corneal epithelial cells and induces programmed cell death
Selective damage to goblet cells: Goblet cells, which secrete mucin (such as MUC5AC), are damaged, reducing tear film stability4)
Tight junction damage: The barrier function of the corneal epithelium declines, increasing sensitivity to outside irritants
Promotion of conjunctival fibrosis: It promotes inflammation and fibrosis in the subconjunctival tissue and affects bleb scarring after trabeculectomy (filtering surgery)5)
Effect on the lipid layer: Its surfactant action destabilizes the tear film lipid layer and worsens MGD
The relationship between BAK concentration and epithelial toxicity is shown below.
It can be reduced. BAK (benzalkonium chloride) is the most commonly used preservative in eye drops, and its toxicity to the corneal epithelium has been confirmed. With long-term use, switching to preservative-free formulations or BAK-free formulations (such as those containing Polyquad) is desirable. The benefit of switching is especially great for patients with dry eye and for those using three or more eye drops long term.
4. Diagnosis and evaluation of preservative toxicity
Allows quantitative assessment of goblet cell density
In vivo confocal microscopy
Evaluates fine structural changes in the corneal epithelium, corneal nerves, and conjunctiva
In the history, be sure to confirm the type and number of eye drops being used, whether they contain BAK, and the length of use. It is also important to check whether the timing of symptom onset matches the start or change of the eye drops.
Allergic conjunctivitis: an allergy to the active ingredient of the eye drop itself (drug component). Papillary reaction and eosinophilic infiltration are marked
Dry eye: may coexist with and worsen BAK toxicity. Distinguish it by evaluating tear volume and tear function
Drug-induced corneal disorder: injury caused by drug components other than BAK. Confirm by the improvement course after stopping the drops
The most important measure in managing BAK toxicity is switching to preservative-free (PF) formulations.
Formulation type
Typical products (examples)
Features
Unit-dose type (single-use)
ムコスタUD® 0.2%,ジクアスUD® 3%,ヒアレインミニ® 0.1%/0.3%
Use up each unit after opening. No preservative needed for long-term storage
Multidose PF type (with built-in filter)
Cosopt® Mini combination eye drops (PF)
Sterile container structure for repeated use
BAK-free alternative preservative formulation
Travatan® (contains Polyquad)
Uses an alternative preservative with lower toxicity than BAK
BAK-free formulation with the same active ingredient
Tapros® PF (tafluprost 0.0015%)
Alternative to latanoprost. Insurance-covered for ocular hypertension and glaucoma
Switching to alternative PF glaucoma eye drops has been reported to significantly improve objective indicators of ocular surface damage (SPK, BUT, and goblet cell density)7, 8).
Using combination eye drops (formulations that combine 2 to 3 ingredients in one bottle) is effective in reducing total BAK exposure9).
Reduction in instillation frequency: Compared with using 2 to 3 single-agent drops, switching to one bottle greatly reduces the number of BAK exposures
Reduction in BAK content: The BAK content in combination eye drops is lower than the total from separate single-agent drops
Punctal occlusion: Pressing the lacrimal sac area (inner corner of the eye) for 1 to 2 minutes after instillation promotes BAK drainage through the nasolacrimal duct and can also reduce systemic absorption
Eye rinsing: Rinsing the eye after instillation can remove BAK remaining on the corneal surface. However, excessive rinsing can dilute the tear film, so caution is needed
For patients scheduled for glaucoma filtering surgery (trabeculectomy or tube shunt surgery), switching to a BAK-free formulation about 2 to 4 weeks before surgery may reduce conjunctival inflammation and improve surgical outcomes5). It is also useful to assess goblet cell density with preoperative conjunctival impression cytology.
If dry eye is caused or worsened by BAK toxicity, add the following treatments.
3% diquafosol sodium eye drops (Diquas®): Promotes mucin secretion through P2Y2 receptors. A preservative-free unit-dose form (Diquas UD®) is also available
2% rebamipide eye drops (Mucosta® ophthalmic solution): In addition to promoting mucin production, it has anti-inflammatory effects. A preservative-free unit-dose form (Mucosta UD®) is available
QHow can the ocular surface be protected when using many eye drops for glaucoma?
A
Combining multiple measures is effective. First, switching to combination eye drops can reduce the number of instillations and lower total exposure to BAK. Next, discuss switching to preservative-free (PF) formulations with your ophthalmologist. Nasolacrimal occlusion after instillation is also effective and can reduce intraocular and systemic absorption of BAK. If dry eye symptoms are present, using mucin-secretion-promoting eye drops such as diquafosol ophthalmic solution (Diquas UD®) or rebamipide ophthalmic solution (Mucosta UD®) together is also effective9).
6. BAK content and alternative formulations of major glaucoma eye drops
Glaucoma requires lifelong eye drop use, and the effects of BAK toxicity are a major concern in this area. The following summarizes the BAK content and alternative formulations of major eye drops.
BAK toxicity is concentration-dependent, and latanoprost (0.02%) carries the highest risk6). When using multiple BAK-containing eye drops, the issue is not the total BAK concentration across the drugs, but repeated exposure of the ocular surface from each drop. Tafluprost (Tapros® PF) has the same intraocular pressure-lowering effect as latanoprost while being BAK-free, and studies in both animals and clinical trials have shown that its impact on the ocular surface is significantly lower6, 7).
Unlike BAK, Polyquad is a polymeric cationic surfactant. Because it has a large molecular weight and low corneal permeability, its epithelial toxicity is low. In vitro studies have also confirmed that its toxicity to ocular surface epithelial cells is significantly lower than BAK8).
SoftZIA® (zinc-containing preservative system): A low-toxicity preservative system that uses zinc ions. Comparative studies with BAK have shown superior corneal tolerability7), and it has been adopted in some glaucoma eye drops
OcuPure® (hydrogen peroxide-based): A preservative that breaks down into oxygen and water after instillation. It leaves almost no residue on the ocular surface and is considered low in toxicity
Chlorhexidine derivatives and polyaminopropyl biguanide (PAPB): The application of low-toxicity preservatives developed for contact lens care products to eye drops is being investigated
Research is also progressing toward eliminating the need for eye drops themselves.
Sustained-release intraocular implants: Sustained-release implants placed in the anterior chamber or vitreous cavity, avoiding both systemic exposure to eye drops and preservative toxicity
Punctal plug DDS: Reports have described attempts to slowly release medication from punctal plugs and greatly reduce the number of eye drops used
For the long-term effects of BAK on the ocular surface, studies using in vivo confocal microscopy have reported a decrease in corneal nerve density. This finding suggests that BAK toxicity affects not only the corneal epithelium but also the corneal nervous system, and further evaluation is needed, including its association with neuropathic pain11). In addition, more evidence is needed on the relationship between long-term BAK use and bleb scarring after glaucoma filtering surgery, including optimizing the preoperative BAK washout period.
Baudouin C, Labbé A, Liang H, et al. Preservatives in eyedrops: the good, the bad and the ugly. Prog Retin Eye Res. 2010;29(4):312-334. doi:10.1016/j.preteyeres.2010.03.001. PMID:20302969.
Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86(4):418-423. doi:10.1136/bjo.86.4.418. PMID:11914211; PMCID:PMC1771067.
Jaenen N, Baudouin C, Pouliquen P, et al. Ocular symptoms and signs with preserved and preservative-free glaucoma medications. Eur J Ophthalmol. 2007;17(3):341-349. doi:10.1177/112067210701700311. PMID:17534814.
Noecker RJ, Herrygers LA, Anwaruddin R. Corneal and conjunctival changes caused by commonly used glaucoma medications. Cornea. 2004;23(5):490-496. doi:10.1097/01.ico.0000116526.57227.82. PMID:15220734.
Broadway DC, Grierson I, O’Brien C, et al. Adverse effects of topical antiglaucoma medication. II. The outcome of filtration surgery. Arch Ophthalmol. 1994;112(11):1446-1454. doi:10.1001/archopht.1994.01090230060021. PMID:7980134.
Liang H, Baudouin C, Pauly A, et al. Conjunctival and corneal reactions in rabbits following short- and repeated exposure to preservative-free tafluprost, commercially available latanoprost and 0.02% benzalkonium chloride. Br J Ophthalmol. 2008;92(9):1275-1282. doi:10.1136/bjo.2008.138768. PMID:18723745; PMCID:PMC2569147.
Kahook MY, Noecker RJ. Comparison of corneal and conjunctival changes after dosing of travoprost preserved with sofZia, latanoprost with 0.02% benzalkonium chloride, and preservative-free artificial tears. Cornea. 2008;27(3):339-343. doi:10.1097/ICO.0b013e31815cf651. PMID:18362664.
Ammar DA, Noecker RJ, Kahook MY. Effects of benzalkonium chloride-preserved, polyquad-preserved, and sofZia-preserved topical glaucoma medications on human ocular epithelial cells. Adv Ther. 2010;27(11):837-845. doi:10.1007/s12325-010-0070-1. PMID:20931366.
Martone G, Frezzotti P, Tosi GM, Traversi C, Mittica V, Malandrini A, et al. An in vivo confocal microscopy analysis of effects of topical antiglaucoma therapy with preservative on corneal innervation and morphology. Am J Ophthalmol. 2009;147(4):725-735.e1. doi:10.1016/j.ajo.2008.10.019.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.