In primary gaze, the upper eyelid margin is normally 1 to 2 mm below the superior limbus of the cornea. Upper eyelid retraction refers to a state in which sclera can be seen between the upper eyelid margin and the superior limbus. MRD-1 (distance from the corneal light reflex to the upper eyelid margin) is used as a guide when it exceeds 5.5 mm. Lower eyelid retraction is assessed as an increase in MRD-2. When eyelid retraction occurs, corneal exposure becomes a problem, and surgery may be needed in addition to symptomatic treatment.
Eyelid retraction is the most common sign of thyroid eye disease (TED)6). The incidence of TED is estimated at 16/100,000 women/year and 2.9/100,000 men/year1). The age of onset shows a bimodal pattern in the 40s to 50s and 60s to 70s3), and smoking is known as an important risk factor5). More than half of patients with thyroid eye disease are estimated to have eyelid retraction, which has a major impact on quality of life in both visual function and appearance1).
Eyelid retraction (MRD-1 > 5.5 mm) and ptosis (MRD-1 < 3.5 mm) are opposite conditions. In thyroid eye disease, eyelid retraction occurs in the affected eye, while with unilateral ptosis, the opposite eyelid may appear relatively retracted because of Hering’s law. Distinguishing this from pseudoretraction is essential when deciding on treatment.
QWhat is the difference between eyelid retraction and ptosis?
A
Eyelid retraction is a state in which the MRD-1 exceeds 5.5 mm and the upper eyelid sits higher than usual, which is the opposite of ptosis (MRD-1 < 3.5 mm). In thyroid eye disease, eyelid retraction is the most common sign, whereas ptosis is most often caused by age-related aponeurotic degeneration. It is also important to note that, because of Hering’s law, ptosis in one eye can cause pseudoretraction in the other eye.
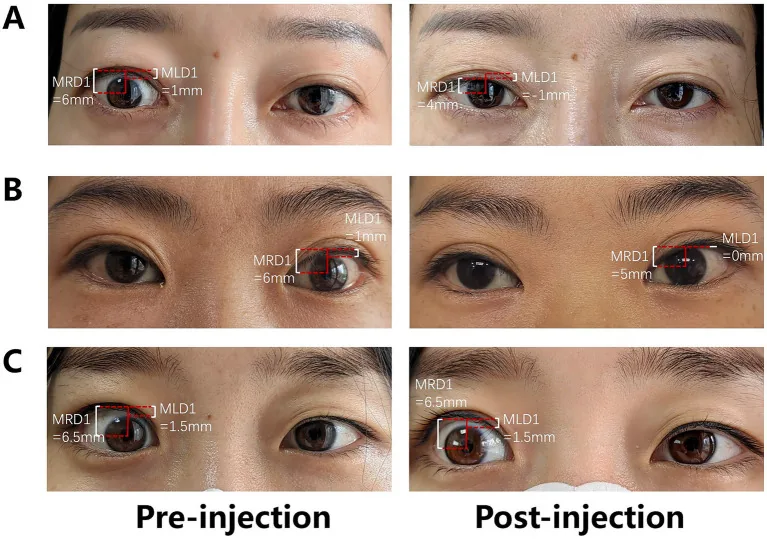
Zheng W, et al. Percutaneous para-levator palpebrae superioris and subconjunctival injection of triamcinolone acetonide for upper eyelid retraction in thyroid-associated ophthalmopathy. Front Med (Lausanne). 2025;12:1679057. DOI: 10.3389/fmed.2025.1679057. Figure 2. License: CC BY. PMCID: PMC12457333.
Anterior segment photographs before injection (left column) and after injection (right column) in three cases. Before injection, MRD1 is 6–6.5 mm, exceeding the reference value (5.5 mm), and sclera is visible above the upper limbus of the cornea (scleral show). Each panel is labeled in a red box with MRD1 and MLD1 together with the measured values. This corresponds to the increased MRD1 and scleral show discussed in the ‘Main symptoms and clinical findings’ section.
The course of thyroid eye disease follows the Rundle curve, transitioning from an active inflammatory phase to a stable phase 6). In the early stage, dryness and irritation around the eyes are the main symptoms; in the middle stage, eyelid retraction, proptosis, and diplopia become apparent, and in severe cases, corneal exposure and compressive optic neuropathy may occur 3). The Clinical Activity Score (CAS) is used to assess inflammatory activity, and a score of 3 or more out of 7 is considered the active phase 1).
Mechanism: Inflammatory fatty infiltration of the levator palpebrae superioris → muscle cell necrosis and scarring + abnormal sustained contraction due to sympathetic overactivity of the Müller muscle.
Features: Can affect both eyes or one eye. Can occur even when thyroid function is normal.
In the severity classification by EUGOGO (European Group on Graves’ Orbitopathy), cases are classified into three levels: mild, moderate to severe, and sight-threatening1). In the NOSPECS classification, severity is assessed from classes 0 to 6, and the presence or absence of extraocular muscle involvement, corneal involvement, and optic nerve involvement determines the severity4). Sight-threatening cases (compressive optic neuropathy or corneal breakdown) are candidates for urgent intervention.
MRD-1 measurement is the basic quantitative method for upper eyelid retraction. Measure the distance from the central corneal light reflex to the upper eyelid margin, and if it exceeds 5.5 mm, judge it as upper eyelid retraction. To exclude frontalis compensation, lightly stabilize the forehead during measurement. MRD-2 is the distance from the central corneal light reflex to the lower eyelid margin, and it is used to evaluate lower eyelid retraction.
Hertel exophthalmometer values below 18 mm are considered normal, but in TED patients they often exceed 21 mm3). The degree of proptosis tends to correlate with the severity of eyelid retraction.
Evaluate superficial punctate keratitis (SPK) with fluorescein staining. SPK that matches the exposed area on the lower cornea caused by lagophthalmos is characteristic, and it is used to judge the need for treatment and the level of urgency.
If thyroid eye disease is suspected, perform orbital imaging with MRI or CT. On CT, spindle-shaped enlargement of the extraocular muscles is characteristic, and a TED-specific pattern is enlargement of the muscle belly with preservation of the tendon insertion4). MRI is useful for evaluating the Müller muscle and levator palpebrae superioris, and for assessing inflammatory activity (high signal on T2-weighted images). If a midbrain-related cause is suspected, perform head MRI/CT to rule out pineal tumor and hydrocephalus.
Thyroid function tests (FT4, FT3, TSH) and autoantibody tests (TRAb, TSAb, TgAb, TPOAb) are performed. Some patients with eyelid retraction may have TED even when thyroid function is normal, so checking autoantibodies is essential6).
Clinical diagnosis is the basis, and the triad of eyelid retraction + proptosis + diplopia strongly suggests TED6).
Pseudo-upper eyelid retraction due to Hering’s law: differentiate by observing the contralateral ptosis while covering one eye.
Parinaud syndrome: a combination of upgaze palsy + eyelid retraction (Collier’s sign). Intracranial evaluation is essential.
Drug-induced (sympathomimetics, etc.): confirm the medication history.
Voluntary eyelid retraction: evaluate for psychiatric background.
QWhat is the difference between Dalrymple sign and von Graefe sign?
A
Dalrymple sign is widening of the palpebral fissure in the primary position (straight-ahead gaze), with sclera exposed above the superior corneal limbus. Von Graefe sign is delayed following of the upper eyelid during downgaze (lid lag). Both are characteristic findings of thyroid eye disease and are used together with MRD-1 measurement to diagnose eyelid retraction and assess severity.
Steroid treatment is effective for eyelid retraction caused by inflammation.
Local injection: Local injection of triamcinolone acetonide (Kenacort-A® 1 ampule) is effective for upper eyelid edema and inflammatory eyelid retraction.
Steroid pulse therapy: Indicated during the inflammatory phase; one course consists of methylprednisolone 1 g for 3 days.
Intravenous steroids (IV methylprednisolone): Administering 500–1000 mg once weekly for 6–12 weeks is more effective than oral steroids5). It is indicated for moderate to severe TED in the active inflammatory phase (CAS ≥ 3).
In recent years, biologics for TED have become available.
Teprotumumab (IGF-1R inhibitor): In a phase 2 trial2) and phase 3 RCT7) in moderate to severe active TED, significant improvement in proptosis and diplopia was shown. Improvement in eyelid retraction has also been reported, making it a promising treatment option during the active inflammatory phase.
Rituximab (anti-CD20 monoclonal antibody): Use in moderate to severe TED has been reported to reduce disease activity3). It suppresses inflammation through immunosuppression targeting B cells.
Tocilizumab (IL-6 receptor inhibitor): Reported to be beneficial in steroid- and rituximab-refractory cases3).
Timing of surgery: Plan surgery during the inactive phase, after the inflammatory phase has settled and the disease has reached a plateau on the Rundle curve. In general, inflammation stabilizes 1 to 3 years after onset.
Choice of procedure:
Müller muscle excision (Müller muscle resection): Relieves sympathetic overactivity of the Müller muscle. Used for relatively mild eyelid retraction. Good outcomes have been reported with a combination of Müller muscle resection and levator recession6).
Upper eyelid levator recession: The levator aponeurosis complex is recessed to narrow the palpebral fissure. Used for moderate to severe eyelid retraction.
Upper eyelid levator lengthening: The levator aponeurosis is lengthened using a spacer (autologous tissue or artificial material). Used for severe eyelid retraction.
Botulinum toxin preparation (Botox®) injection: Temporarily reduces eyelid retraction by injection into the upper eyelid or above the superior rectus muscle. Used as a bridge before surgery or for temporary control during active inflammation.
Orbital decompression by removing bone from the medial wall or floor of the orbit is performed for severe proptosis and compressive optic neuropathy5). It is not a primary indication for eyelid retraction alone, but eyelid retraction may improve as proptosis decreases.
Smoking cessation: Smoking contributes to worsening severity and treatment resistance in thyroid eye disease, so smoking cessation guidance is recommended5).
Selenium supplementation: In mild thyroid eye disease (TED), selenium supplementation (200 μg/day for 6 months) has been reported to help improve disease activity5).
Stabilization of thyroid function: Keeping thyroid levels normal helps reduce disease severity5).
QWhen can eyelid retraction in thyroid eye disease be treated surgically?
A
Plan surgery after the inflammatory (active) phase has settled and the condition is stable in the inactive phase. Usually, wait until the Rundle curve reaches a plateau (about 1 to 3 years after onset). Surgery is best when the CAS (clinical activity score) is stable and below 3. Surgery during the active inflammatory phase increases the risk of postoperative changes and recurrence.
6. Pathophysiology and detailed disease mechanisms
Eyelid retraction in thyroid eye disease is caused by a combination of two changes: in the upper eyelid levator muscle and the Müller muscle.
Pathology of the upper eyelid levator muscle: inflammatory cell infiltration → fat tissue invading between muscle fibers → muscle cell necrosis and scarring → reduced levator function. As the muscle tissue is pulled tight backward, the eyelid retracts upward.
Pathology of Müller muscle: Müller muscle, a sympathetic smooth muscle, undergoes abnormal sustained contraction in the hyperadrenergic state caused by hyperthyroidism. This lifts the tarsus upward and widens the palpebral fissure.
The core of TED is activation of orbital fibroblasts by autoantibodies against the TSH receptor (TSHR)4). CD4+ and CD8+ T cells infiltrate the orbital tissue and trigger an inflammatory response5), and activated orbital fibroblasts differentiate into adipocytes and myofibroblasts5). Differentiation into adipocytes leads to enlargement of orbital fat, while differentiation into myofibroblasts causes fibrosis of the extraocular muscles and levator muscle.
Increased production of hyaluronic acid (GAG) causes fluid retention and swelling in the orbital tissues5). Inflammatory cytokines such as TNF-α, IL-6, and IL-1β continue to be produced, and tissue injury and fibrosis progress4).
IGF-1 receptor (IGF-1R) forms a complex with TSHR and cooperatively contributes to activation of orbital fibroblasts7). This is the basis for teprotumumab targeting IGF-1R.
Compression of the posterior commissure from dorsal midbrain disease (pineal tumor, hydrocephalus) damages the upper eyelid-depressing neurons of the oculomotor nucleus that innervate the levator palpebrae superioris, causing eyelid retraction. The combination of Collier’s sign (bilateral eyelid retraction) and Parinaud syndrome (upgaze palsy, convergence-retraction nystagmus, and impaired pupillary light reflex) is a characteristic sign complex of dorsal midbrain lesions.
The natural course of thyroid eye disease follows the Rundle curve6), reaching a plateau after 6 to 18 months of the active inflammatory phase after onset and then gradually stabilizing. During the inflammatory phase, eyelid retraction, proptosis, and diplopia fluctuate and progress; in the stable phase, they may improve slightly, but once fibrotic changes are fixed, spontaneous improvement is unlikely.
Treatment of active TED with teprotumumab has shown significant improvement in proptosis and diplopia7), and improvement in eyelid retraction has also been reported. Surgical treatment (levator recession and Müller muscle resection) can achieve stable results when performed during the inactive stable phase. Undercorrection or overcorrection after surgery may require reoperation.
Compressive optic neuropathy (DON) occurs in about 5% of TED patients and requires urgent orbital decompression or high-dose steroid treatment5). Color vision changes, relative afferent pupillary defect (RAPD), and visual field defects are early signs, and regular follow-up is important. Long-standing eyelid retraction and lagophthalmos can cause corneal ulceration and corneal scarring, leading to visual impairment. The impact on quality of life is substantial, with cosmetic concerns, diplopia, and visual dysfunction occurring together1).
QAt what stage is eyelid retraction surgery performed?
A
The usual sequence for orbital and eyelid surgery is: 1) orbital decompression (to reduce proptosis and address optic nerve compression) → 2) strabismus surgery (to correct diplopia caused by fibrosis of the extraocular muscles) → 3) eyelid surgery (to correct eyelid retraction). Because postoperative changes in the earlier steps can affect eyelid position, the next surgery is performed only after stability is confirmed.
Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479. PMID:34297684.
Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the Treatment of Active Thyroid Eye Disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/NEJMoa1910434.
Burch HB, Perros P, Bednarczuk T, et al. Management of thyroid eye disease: a Consensus Statement by the American Thyroid Association and the European Thyroid Association. Eur Thyroid J. 2022;11(6):e220189. doi:10.1530/ETJ-22-0189. https://pmc.ncbi.nlm.nih.gov/articles/PMC9727317/
Dolman PJ. Evaluating Graves’ orbitopathy. Best Pract Res Clin Endocrinol Metab. 2012;26(3):229-248. doi:10.1016/j.beem.2011.11.007.
Bartalena L, Kahaly GJ, Baldeschi L, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-G67. doi:10.1530/EJE-21-0479. PMID:34297684.
Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the treatment of active thyroid eye disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/nejmoa1910434.