Systemic capillary leak syndrome (SCLS) is a rare disorder characterized by transient, severe leakage of fluid and macromolecules from capillaries into tissues. It was first reported by Clarkson in 1960 and is also known as Clarkson disease. Fewer than 500 cases have been reported since 1960 2), with a median age at diagnosis of 48 years and a predominance in older men.
Up to 80% of idiopathic SCLS cases are associated with MGUS (monoclonal gammopathy of undetermined significance, mainly IgG type), but the risk of progression to myeloma is not increased.
Since fluid leakage can occur in any tissue, ophthalmic complications are diverse. Main ocular findings include conjunctival edema, choroidal effusion, and elevated intraocular pressure. Severe cases complicated by acute angle closure and nonarteritic anterior ischemic optic neuropathy (NAION) have also been reported 1).
QHow rare is SCLS?
A
Fewer than 500 cases have been reported worldwide since 1960, making it an extremely rare disease 2). The median age at diagnosis is 48 years, with a predominance in older men. Due to its rarity, diagnosis is often delayed.
Tearing, photophobia, foreign body sensation, itching: Caused by conjunctival edema (chemosis). Vision is often preserved.
Vision loss and eye pain: Reported in cases with choroidal effusion and acute angle closure.
Superior visual field defect: In cases complicated by non-arteritic anterior ischemic optic neuropathy, bilateral symmetric superior arcuate visual field defects become apparent during the recovery phase of SCLS 1).
Clinical Findings (Findings Confirmed by Physician Examination)
Eyelid edema and periorbital edema: Accompanied by facial swelling. May also cause proptosis (due to orbital congestion).
Chemosis: Can become very severe, posing a risk of lagophthalmos and exposure keratopathy. Accompanied by dilation and tortuosity of conjunctival vessels.
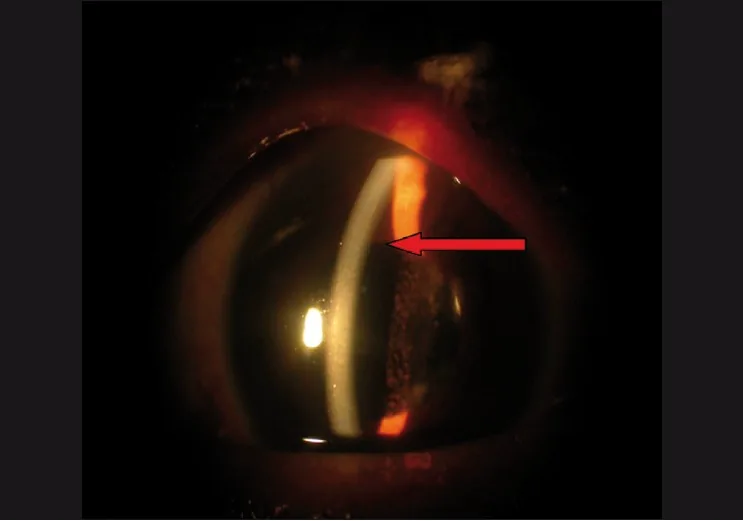
Shallow anterior chamber and angle closure: Caused by anterior rotation of the ciliary body due to ciliary effusion. Not due to a pupillary block mechanism, and can occur even in pseudophakic eyes.
Elevated intraocular pressure: Increased episcleral venous pressure also contributes.
Posterior segment and optic nerve
Choroidal effusion: Caused by decreased colloid osmotic pressure due to a rapid drop in serum albumin. Often bilateral.
Ciliary body effusion: Extensive exudation from the posterior segment to the ciliary body.
In cases complicated by non-arteritic anterior ischemic optic neuropathy, permanent visual field defects may remain. In reported cases, bilateral symmetrical superior arcuate visual field defects were present, but central visual acuity was maintained at 6/7.5 (approximately 0.8) in both eyes1). On the other hand, visual acuity loss due to conjunctival edema, choroidal effusion, and angle closure often recovers with improvement of the systemic condition.
The cause of SCLS is mostly idiopathic (unknown cause). Besides idiopathic, the following triggers have been reported.
Drug-induced: Anticancer drugs such as gemcitabine and clofarabine, monoclonal antibodies, therapeutic growth factors. In clinical trials of denileukin diftitox (a treatment for CTCL), SCLS occurred in 36% of patients9).
Viral infections: Influenza A and B, herpes zoster, dengue fever. In a case report complicated by non-arteritic anterior ischemic optic neuropathy, influenza B was confirmed1).
COVID-19-related: In addition to COVID-19 infection itself, onset has been reported with AstraZeneca, Johnson & Johnson-Janssen, and Pfizer-BioNTech vaccines7)8). The European Medicines Agency (EMA) has recommended that the AstraZeneca vaccine be contraindicated in individuals with a history of SCLS7).
Decompression sickness: SCLS secondary to decompression sickness after diving has been reported6).
Malignancy: SCLS as a paraneoplastic syndrome due to diffuse large B-cell lymphoma (DLBCL), among others3).
Genetic background: A splice site mutation in the TLN1 gene (c.7188+2T>C) has been identified in familial SCLS. It follows an autosomal dominant pattern with incomplete penetrance4).
Risk factors that predispose to non-arteritic anterior ischemic optic neuropathy include hypotension, hemoconcentration, and hypercoagulability due to SCLS, as well as diabetes, hypertension, arteriosclerosis, and a small crowded disc1).
QCan the COVID-19 vaccine cause SCLS?
A
Cases have been reported with both adenovirus vector and mRNA vaccines 7)8). Although a causal relationship has not been established, the EMA recommends that the AstraZeneca vaccine be contraindicated in individuals with a history of SCLS. Those with a history of SCLS should consult their primary care physician before vaccination.
SCLS is a diagnosis of exclusion, based on the presence of capillary leak signs such as generalized edema and refractory hypotension, and the exclusion of other diseases.
The following characteristic laboratory abnormalities are observed in the acute phase.
Hypoalbuminemia (without proteinuria): mean approximately 1.7 g/dL2). In severe cases, albumin levels of 16 g/L5) and 18 g/L8) have been reported.
Hemoconcentration: elevated hematocrit (mean approximately 60%). In severe cases, Ht can reach 69%5) and 72.3%8).
MGUS: detected in up to 80% of cases by serum protein electrophoresis (SPEP). IgG-κ2)5) and IgG-λ1) are common.
Thromboembolism risk: hypercoagulable state due to hemoconcentration. Cases complicated by deep vein thrombosis, inferior vena cava thrombosis8), and pulmonary embolism2) have been reported.
Acute kidney injury (AKI): Occurs in some cases9).
99mTc-HSA scintigraphy can directly demonstrate increased vascular permeability by HSA accumulation in the subcutaneous tissue of the extremities 24 hours after injection9).
Slit-lamp microscopy: Evaluate the degree of conjunctival edema and the presence of shallow anterior chamber or angle closure.
B-mode ultrasound: Confirm the presence and extent of choroidal effusion.
Humphrey visual field test: Detection of superior arcuate visual field defect (in cases with non-arteritic anterior ischemic optic neuropathy)1).
Optical coherence tomography (OCT): Quantitative evaluation of thinning of the inferior retinal nerve fiber layer (in cases with non-arteritic anterior ischemic optic neuropathy)1).
Head and orbital MRI: Used to rule out local infarction or mass lesions1).
Fluid management: Crystalloids are first-line. Excessive fluid resuscitation increases the risk of pulmonary edema and compartment syndrome. Consider high-molecular-weight colloids only when systolic blood pressure is below 70 mmHg as part of a “permissive hypotension” strategy 6).
Vasopressors: Use norepinephrine, etc.
Systemic steroids/IVIG (acute phase): IVIG is administered at 1–2 g/kg/day for 2–3 days.
Thromboembolism prophylaxis: Implement prophylactically for hypercoagulable states due to hemoconcentration.
The main options for attack prevention are shown below.
IVIG (intravenous immunoglobulin): Regular administration of up to 2 g/kg/month. In SCLS patients with MGUS, the IVIG group had a 5-year survival rate of 91% and a 10-year survival rate of 77%, compared to 47% and 37% in the non-IVIG group, respectively, showing a significant difference. The median annual attack frequency under IVIG treatment was 0 (range 0–3.3)8).
β2-agonists (terbutaline) + theophylline: Used to suppress endothelial permeability by increasing cAMP. Terbutaline 5 mg three times daily, theophylline 400–1600 mg/day6). However, the median annual attack frequency under treatment was 2.25 (range 0–20), which is inferior to IVIG8).
Methylprednisolone pulse + IVIG combination: Administration of mPSL 1000 mg/day for 3 days + IVIG 1 g/kg has been reported8).
QWhat is the most effective treatment for preventing attacks of SCLS?
A
Monthly administration of IVIG (intravenous immunoglobulin) is considered the most effective. The 5-year survival rate in the IVIG group is 91%, compared to 47% in the non-IVIG group, a large difference. The median annual attack frequency in the IVIG group is 0, showing excellent suppression8).
Choroidal/ciliary body effusion: Systemic and topical (eye drops, periocular) steroids are used and are effective in some reports. Some case series show poor response.
Intraocular pressure management: Use topical intraocular pressure-lowering medications.
Conjunctival edema/exposure keratopathy: Lubrication with artificial tears. In severe cases, temporary tarsorrhaphy may be considered, but there is a risk of compressing the orbit and causing orbital compartment syndrome.
Angle closure: Laser peripheral iridotomy (LPI) or cataract surgery may be considered, but caution is needed because angle closure can persist due to ciliary body effusion even in pseudophakic eyes.
Surgery/laser for choroidal effusion: Usually resistant. There is no established surgical treatment for SCLS.
The final common pathway of SCLS is vascular endothelial dysfunction. The intercellular gaps between endothelial cells widen, leading to leakage of macromolecules and extravasation of water.
The following changes are observed during an attack:
Increased IL-2 receptor expression on mononuclear cells, increased production of CXCL10, CCL2, IL-1β, IL-8, and IL-12
Increased CD8+/CD25+ T cell concentration, increased TNF-α expression
Increased VEGF-D5)
Elevated VEGF and angiopoietin-2 during attacks5)
In in vitro models, angiopoietin-2 inhibitors and IVIG significantly reduced endothelial permeability, whereas bevacizumab (a VEGF inhibitor) had minimal effect 5).
TLN1 gene mutation and endothelial barrier disruption
Elefant et al. (JCI Insight, 2024) identified a heterozygous splice mutation (c.7188+2T>C) in the TLN1 gene in three patients with familial SCLS 4). This mutation causes in-frame skipping of exon 54, destabilizing the talin1 R13 domain. Dysfunction of the C-terminal actin-binding site (ABS3) leads to markedly reduced junctional localization of VE-cadherin, fragmentation of adherens junctions (AJ) and tight junctions (TJ), and increased endothelial barrier permeability. Upon thrombin stimulation, SCLS mutant endothelium showed approximately four times greater FITC-dextran permeability than controls.
Denileukin diftitox binds to cells expressing the IL-2 receptor and inhibits protein synthesis through internalization of a diphtheria toxin fragment. SCLS is thought to be caused by both increased vascular permeability (IL-2R effect) and inhibition of protein synthesis (diphtheria toxin effect) 9).
Choroidal effusion: Caused by decreased colloid osmotic pressure due to a rapid drop in serum albumin.
Ciliary effusion and angle closure: Ciliary effusion → forward rotation of the ciliary body → shallow anterior chamber and angle closure. Since it is not due to a pupillary block mechanism, it can occur even in pseudophakic eyes.
Elevated intraocular pressure: In addition to angle closure, increased episcleral venous pressure also contributes.
Non-arteritic anterior ischemic optic neuropathy: Hypotension plus hypercoagulability → segmental infarction of the optic disc via the posterior ciliary arteries. Because the posterior ciliary arteries form end arteries and a watershed zone, optic disc infarction is prone to occur during shock 1).
7. Latest research and future perspectives (reports at the research stage)
Elefant et al. (2024) showed that in endothelial cells expressing SCLS mutant talin1, restoration of normal splicing by splice-switching antisense oligonucleotides could be proposed as a therapeutic strategy 4). If VE-cadherin junctional localization and AJ integrity are restored, it may lead to repair of endothelial barrier function.
Elevated VEGF-D levels have been recorded in SCLS patients, and the VEGFR3-mediated pathway has been proposed as a future therapeutic target. Anti-VEGF therapy (intravenous bevacizumab) was attempted in one case but no clinical response was obtained. Meanwhile, angiopoietin-2 inhibitors significantly reduced endothelial permeability together with IVIG in in vitro models, but clinical reports are limited 5).
Causal Relationship Research on COVID-19 Vaccine-Associated SCLS
Cases have been reported with both mRNA vaccines and adenovirus vector vaccines7)8), but the causal relationship has not been established, and further research is needed.
Neo YN, Sobti M, Zambarakji H. Bilateral simultaneous non-arteritic ischaemic optic neuropathy: a rare complication of idiopathic systemic capillary leak syndrome (SCLS). BMJ case reports. 2021;14(5). doi:10.1136/bcr-2021-242847. PMID:33947680; PMCID:PMC8098958.
Correia RS, Dos Santos DP, Delgado M. Idiopathic Systemic Capillary Leak Syndrome: A Clinical Case. Cureus. 2023;15(12):e50301. doi:10.7759/cureus.50301. PMID:38205445; PMCID:PMC10776458.
Silva B, Gaspar V, Alves C, Andrade MI, Chinchilla Mata J. Systemic Capillary Leak Syndrome as a Paraneoplastic Syndrome. Cureus. 2024;16(5):e60923. doi:10.7759/cureus.60923. PMID:38910633; PMCID:PMC11193439.
Elefant N, Rouni G, Arapatzi C, Oz-Levi D, Sion-Sarid R, Edwards WJ, et al. Talin1 dysfunction is genetically linked to systemic capillary leak syndrome. JCI insight. 2024;9(24). doi:10.1172/jci.insight.173664. PMID:39704176; PMCID:PMC11665552.
Bouchlarhem A, Lamzouri O, El aidouni G, et al. Consider systemic capillary leak syndrome in monoclonal gammopathy with shock. Ann Med Surg. 2021;72:103013.
Mathavan A, Mathavan A, Jones K, Ataya A. Systemic capillary leak syndrome secondary to decompression sickness. BMJ case reports. 2023;16(7). doi:10.1136/bcr-2022-253045. PMID:37407231; PMCID:PMC10335547.
Yang C, Tsang MY, Zypchen LN, Luong C. Pericardial effusion and systemic capillary leak syndrome late post-SARS-CoV-2 vaccination. BMJ case reports. 2023;16(10). doi:10.1136/bcr-2023-256527. PMID:37813549; PMCID:PMC10565171.
Inoue M, Yasue Y, Kobayashi Y, Sugiyama Y. Systemic capillary leak syndrome (SCLS) after receiving BNT162b2 mRNA COVID-19 (Pfizer-BioNTech) vaccine. BMJ case reports. 2022;15(3). doi:10.1136/bcr-2022-248927. PMID:35292552; PMCID:PMC8928276.
Horino T, Okada D, Inotani S, Nakajima H, Komori M, Terada Y. Denileukin diftitox-induced systemic capillary leak syndrome with acute kidney injury. CEN case reports. 2023;12(1):63-67. doi:10.1007/s13730-022-00720-3. PMID:35870043; PMCID:PMC9892406.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.