Cutaneous T-cell lymphoma (CTCL) is a group of non-Hodgkin lymphomas in which malignant T lymphocytes infiltrate the skin. It accounts for approximately 4% of all non-Hodgkin lymphomas and is twice as common in men. The average age of onset is 50–60 years.
The most common subtype is mycosis fungoides (MF), which accounts for 60% of CTCL cases 1). Sézary syndrome (SS) is an aggressive variant of MF, accounting for 5%, characterized by the triad of erythroderma, lymphadenopathy, and Sézary cells in the blood.
CTCL presents as erythematous patches, plaques, and tumors, accompanied by pruritus, scaling, and ulceration. It often follows a chronic, low-grade course with relapses and remissions 1). Early MF resembles atopic dermatitis or psoriasis, making early diagnosis difficult 1).
Only about 2% of CTCL patients have ocular abnormalities, but eyelid and periorbital lesions have been reported in advanced stages. Ocular manifestations include seborrheic blepharoconjunctivitis, cicatricial ectropion, meibomianitis, chalazion, and madarosis.
QWhat is the difference between mycosis fungoides (MF) and Sézary syndrome (SS)?
A
Mycosis fungoides (MF) is the most common subtype, accounting for 60% of CTCL, starting with erythematous patches and plaques, and progressing to tumors or erythroderma 1). Sézary syndrome (SS) is an aggressive variant of MF, presenting with the triad of erythroderma, lymphadenopathy, and Sézary cells (atypical T cells with cerebriform nuclei) in the blood. SS follows a more aggressive clinical course.
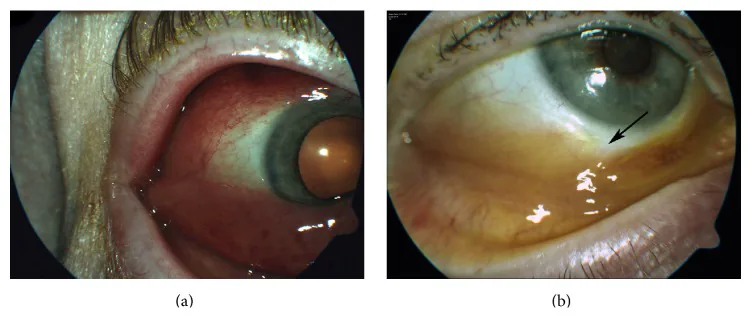
Sultan S Aldrees, Pablo Zoroquiain, Sarah A Alghamdi, Patrick T Logan, et al. Conjunctival Involvement of T-Cell Lymphoma in a Patient with Mycosis Fungoides 2016 Feb 18 Case Rep Ophthalmol Med. 2016 Feb 18; 2016:4786498 Figure 1. PMCID: PMC4775785. License: CC BY.
Slit-lamp image of the right eye. (a) Reddish fleshy tumor, prominent in the lower conjunctiva. (b) After treatment, the lesion has markedly reduced. Note the scar at the biopsy site (arrow).
Seborrheic blepharoconjunctivitis: the most common ocular symptom in CTCL. It involves inflammation and scaling of the eyelid margin.
Cicatricial ectropion: scarring of the anterior lamella due to chronic inflammation and degenerative changes. The lower eyelid margin turns outward. This finding suggests SS.
Meibomianitis: inflammatory obstruction of the meibomian glands. It occurs as an inflammatory lesion of the eyelid.
Other Ocular Symptoms
Chalazion: an eyelid mass due to obstruction of the meibomian or Zeis glands. It can be recurrent.
Madarosis: reflects tumor infiltration or severe inflammation of the eyelid margin. It is an important sign suggesting malignancy.
Eyelid plaques and tumors: Presenting with diffuse thickening, edema, and poikiloderma-like changes.
In early CTCL patients, eyelid lesions may mimic benign dermatitis. CTCL has been reported to have a tendency to localize at sites of previous trauma or surgical scars, potentially exacerbating scars and leading to ectropion.
There have also been reports of peripheral T-cell lymphoma cases where bulbar conjunctival lesions were the only initial symptom.
QHow common are ocular symptoms in CTCL?
A
In a 15-year retrospective study, only about 2% of CTCL patients had at least one disease-related ophthalmic abnormality. However, in advanced stages, the frequency of eyelid and periorbital lesions increases. Ocular symptoms are easily overlooked, and CTCL should be considered in cases of persistent blepharitis or treatment-resistant eyelid lesions.
The exact etiology of CTCL is unknown, but genetic predisposition, environmental factors, and viral infection are suspected. Dysregulation of T-cell function and immune surveillance is the essence of the disease.
In early stages, Th1 cells and CD8-positive cells suppress the proliferation of malignant CD4-positive cells. In advanced stages, defects in Th1 signaling and a decrease in regulatory cells lead to proliferation of malignant T cells and a predominance of Th2-type immune response.
Skin biopsy and histopathological examination: Detection of atypical T cells with CD4-positive cerebriform nuclei, epidermotropism, and Pautrier microabscesses 1)
Immunophenotyping: Analysis of T-cell surface markers.
Molecular biological testing: Identification of monoclonal rearrangement of T-cell receptor genes.
Clinical staging: Scoring tools such as mSWAT and CLIPi.
Non-surgical correction with hyaluronic acid filler injection is also being considered. This technique stretches the adherent skin and corrects anterior lamellar shortening, with effects lasting 12 to 18 months.
Management of Meibomian Gland Inflammation and Chalazion
Treatment of cicatricial ectropion is primarily surgical repair. It combines scar release with Z-plasty, myocutaneous flaps, or full-thickness skin grafts, along with correction of eyelid laxity using the lateral tarsal strip procedure. Non-surgical approaches such as hyaluronic acid filler injection have also been reported. This corrects anterior lamellar shortening by stretching the adherent skin, with effects lasting 12 to 18 months. However, if CTCL is the underlying cause, eyelid lesions may improve with systemic treatment, so multidisciplinary treatment planning is important.
CTCL has a multifactorial pathogenesis, with genetic, epigenetic, and immunological factors contributing to clonal proliferation of malignant T cells. In the early stage, benign Th1 cells and CD8-positive cells suppress the proliferation of a small number of malignant CD4-positive cells.
In the advanced stage, defects in Th1 signaling and a decrease in benign regulatory cells accelerate the proliferation of malignant T cells. A Th2-dominant immune response emerges, leading to a reduction in healthy T cells and NK cells, resulting in immune surveillance failure.
Infiltration of malignant T cells into the eyelids causes chronic inflammation, leading to seborrheic blepharoconjunctivitis and meibomianitis. Chronic inflammation results in scarring and degenerative changes of the anterior lamella, causing cicatricial ectropion.
CTCL has been reported to have a tendency to localize at sites of previous trauma or surgical scars, potentially worsening existing scars and promoting ectropion. Eyelash loss reflects hair follicle destruction due to tumor infiltration or severe inflammation at the eyelid margin.
CTCL generally follows a chronic, low-grade course, but treatment resistance is a problem 1). Recurrence occurs in the majority of cases 1). Ocular symptoms may improve with systemic treatment, but if left untreated, there is a risk of corneal exposure, ulceration, and vision loss due to cicatricial ectropion.
Early detection and management by a multidisciplinary team lead to the best ophthalmic outcomes.
Ojeaburu L, Larsen T. Mycosis Fungoides. Brown Hospital Medicine. 2023;2(4). doi:10.56305/001c.85106.
Day A, Abramson AK, Patel M, Warren RB, Menter MA. The spectrum of oculocutaneous disease: Part II. Neoplastic and drug-related causes of oculocutaneous disease. J Am Acad Dermatol. 2014;70(5):821.e1-19. PMID: 24742849.