Demodex blepharitis is a chronic inflammation of the eyelid margin caused by overpopulation of mites of the genus Demodex, which normally inhabit human hair follicles and sebaceous glands. It can present as either anterior blepharitis (centered on the eyelash base) or posterior blepharitis (centered on the meibomian glands). Cylindrical dandruff surrounding the eyelash base is a sign with high pathological significance and serves as a starting point for clinical diagnosis1)2).
Marginal blepharitis is a chronic inflammation of the eyelash roots and glands at the eyelid margin, classified into staphylococcal (ulcerative) blepharitis, seborrheic blepharitis, posterior blepharitis (MGD), and mixed types. Demodex blepharitis is a subtype that can overlap with any of these and has historically been recognized more as “one of the causes” rather than an independent disease.
The genus Demodex was first described by Henle in 1842, and in 1963, Post and Juhlin reported its association with human blepharitis1). For a long time, the degree of pathogenicity was debated, but epidemiological studies, immunological analyses, and treatment response evaluations since the 2000s have increasingly clarified its direct involvement in a certain number of cases of chronic blepharitis, recurrent chalazion, and blepharokeratoconjunctivitis1)6).
There are two main species of Demodex that parasitize humans.
Demodex folliculorum: Body length 0.3–0.4 mm. It parasitizes in clusters within hair follicles, including those of eyelashes. It feeds on keratinocytes and is considered a primary cause of anterior blepharitis at the eyelid margin1)6).
Demodex brevis: Body length approximately 0.2 mm. It tends to parasitize singly within the ducts of meibomian glands and Zeis glands, causing posterior blepharitis and MGD-like findings1)5)6).
Both species have a life cycle of approximately 14–18 days, mating on the skin surface at night and developing from eggs to larvae to adults1).
The prevalence of Demodex infestation increases markedly with age1).
Ages 20–30: approximately 20–30%
Ages 60 and older: over 80%
Ages 70 and older: nearly 100%
Demodex infestation is found in approximately 30–74% of patients with chronic blepharitis1). In the United States, the estimated number of patients with Demodex blepharitis is about 25 million, with reports that 80% of patients experience interference with daily life, 47% have difficulty driving at night, and 34% face restrictions in contact lens wear or makeup use1).
In a Japanese population-based study (Hirado-Takushima Study), the prevalence of MGD was reported as 21.6% in the 40s, 41.9% in the 60s, and 63.9% in the 80s4). Since MGD and Demodex overlap in pathophysiology, it has been suggested that Demodex may be involved in a certain proportion of these elderly individuals4).
There is no internationally unified official diagnostic criteria yet. In Japan, diagnostic criteria as an independent disease have not been established, and clinical judgment is made within the framework of chronic blepharitis and MGD1)4).
QHow common is Demodex blepharitis?
A
Demodex infestation is confirmed in approximately 30–74% of patients with chronic blepharitis, and it is estimated that there are about 25 million potential patients in the United States1). The infestation rate increases with age: 20–30% in the 20s, over 80% in those aged 60 and older, and nearly 100% in those aged 70 and older1). In a Japanese population survey, the prevalence of MGD was 21.6% in the 40s, 41.9% in the 60s, and 63.9% in the 80s, and Demodex is thought to be involved in some of these cases4).
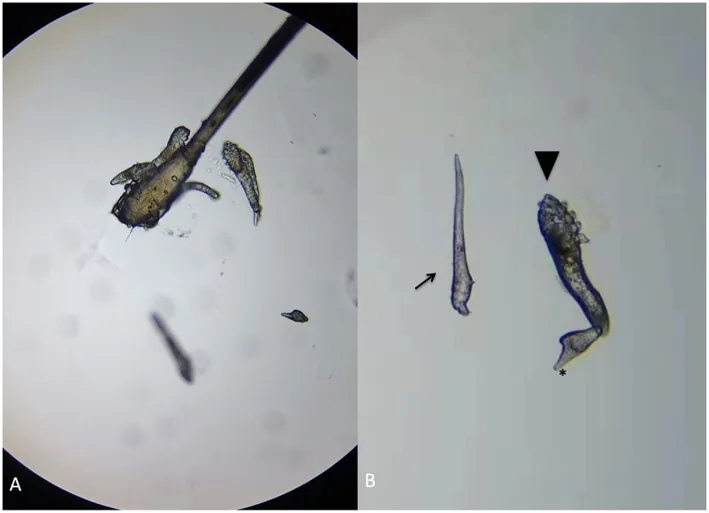
Huo Y, et al. First case of Phthirus pubis and Demodex co-infestation of the eyelids: a case report. BMC Ophthalmol. 2021. Figure 2. PMCID: PMC7937296. License: CC BY.
Microscopic findings of Demodex in the patient’s right eye: (a) a cluster of mites and eggs associated with eyelash follicles, (b) eggs (arrow), larvae with three pairs of legs (arrowhead), and adults with four pairs of legs (*). This corresponds to the detection of mites by microscopic examination discussed in the section “2. Main Symptoms and Clinical Findings.”
Typical complaints include chronic itching, burning sensation, and foreign body sensation at the eyelid margin. Itching tends to be stronger in the morning and at night, and patients often describe it as “the edge of the eye feels itchy” or “the base of the eyelashes tingles”1). It may be accompanied by discharge, tearing, photophobia, and blurred vision, with symptoms recurring in cycles of remission and exacerbation.
The impact on quality of life in patients with Demodex blepharitis is not insignificant. According to reports, 80% of patients experience effects on daily life, 47% have difficulty driving at night, and 34% have restrictions on contact lens use or makeup1). Complaints such as a feeling of eyelash clumping, eyelash loss, and makeup coming off easily are also characteristic1).
The diagnosis of Demodex blepharitis is primarily based on observation using a slit lamp microscope with a diffuser. The following findings are noted1)2)4).
Cylindrical dandruff (CD): Transparent to white hard collar-like scales surrounding the base of the eyelashes. This is a strong suggestive finding of Demodex infestation and has the highest diagnostic value1)2)
Eyelid margin redness and telangiectasia
Eyelash loss, misdirection, and irregular arrangement
Meibomian gland orifice obstruction (plugging, pouting, ridge), irregular arrangement, anterior or posterior displacement of the mucocutaneous junction, and eyelid margin irregularity4)
Conjunctival hyperemia and punctate superficial keratopathy
Meibum qualitative abnormality of grade 2 or higher on the Shimazaki classification4)
Lee et al. analyzed 9 cases of Demodex blepharitis and detected D. folliculorum in all cases. Notably, the cases included children aged 5, 13, and 14 years, who presented with severe blepharokeratoconjunctivitis (BKC) accompanied by corneal ulcers and corneal neovascularization2). In recurrent childhood keratitis, involvement of Demodex should be suspected.
Zhang and Liang reported a case of a 46-year-old man. The patient presented with a one-month history of decreased visual acuity in the right eye, and examination revealed dandruff at the eyelash roots, eyelid margin telangiectasia, meibomian gland orifice obstruction, and punctate superficial keratopathy5). Demodex was not detected in epilated eyelashes, but after antiseptic treatment of the eyelid margin, meibum was expressed and examined under a microscope, revealing 15 D. brevis organisms. Symptoms improved with eyelid hygiene using tea tree oil. This case demonstrates the existence of Demodex blepharitis where D. brevis resides only within the meibum without external findings5).
Note: Even with mild external findings, D. brevis may be hidden in meibum; consider active detection tests in treatment-resistant cases
QWhat is cylindrical dandruff?
A
Cylindrical dandruff is a transparent to white hard scale that adheres like a collar around the base of the eyelashes1). When Demodex proliferates in hair follicles, host keratinocytes reactively hyperkeratinize, and the formed keratin adheres to the base of the eyelashes along with mite feces and debris1). Although similar in shape to collarettes seen in staphylococcal blepharitis, cylindrical dandruff is considered a highly specific finding for Demodex infestation, and its presence provides strong evidence to suspect Demodex involvement1)2).
Demodex folliculorum and Demodex brevis are both ectoparasites that commonly inhabit human skin, and are found in a certain proportion of healthy individuals1)6). The differences between the two are summarized below.
The following factors have been reported to be involved in Demodex overinfestation and blepharitis1)4)6).
Aging: Infestation rate increases with age, and nearly all individuals over 70 years old are infested1).
Rosacea: In patients with cutaneous rosacea, Demodex density is several times higher than in healthy individuals. Ocular rosacea is an important background for Demodex blepharitis1).
Meibomian gland dysfunction (MGD): Demodex is considered a risk factor for MGD, and the two conditions mutually exacerbate each other4).
Immunosuppression: Infestation density increases in patients with HIV infection, diabetes, long-term steroid use, or chemotherapy1).
There are histopathological reports of Demodex folliculorum observed within the meibomian glands, and epidemiological studies suggesting an association between Demodex and MGD. However, many aspects of the causal relationship and contribution to pathology remain unclear4).
QDoes everyone have Demodex?
A
Yes. Demodex folliculorum and Demodex brevis are common ectoparasites of human skin, and a certain number are present in most healthy adults1). Although the infestation rate is low in young people, it increases with age, and reports indicate that nearly all individuals over 70 years old have Demodex1). It becomes pathological only when excessive infestation causes physical obstruction, inflammatory reactions, or ocular surface damage; the presence of Demodex itself does not signify disease1)6).
The diagnosis of Demodex blepharitis is made by combining clinical findings (especially cylindrical dandruff) with direct detection of Demodex. There are no internationally unified official diagnostic criteria yet, and comprehensive judgment including treatment response is necessary1).
Inquire about chronic itching of the eyelid margin (especially worsening in the morning), foreign body sensation, madarosis, history of recurrent chalazion, presence of rosacea, and poor response to previous blepharitis treatments. Also check for use of cosmetics, contact lenses, eyelash extensions, and history of hot springs or pool use.
Technique: Epilate about 4 eyelashes from each upper and lower eyelid, and observe under a light microscope with a coverslip. In a study by Lee et al., adult and larval D. folliculorum were identified in all 9 cases2).
Diagnostic criteria: Many reports consider 2 or more mites per 4 eyelashes as pathological1).
Limitations: D. brevis parasitizes deeper layers (meibomian glands) than hair follicles, so it may not be detected by eyelash epilation1)5).
Direct observation of meibum
Technique: After antiseptic treatment of the eyelid margin, express meibum by compressing the tarsal plate, collect it on a glass slide, and observe under a microscope.
Utility: Zhang and Liang detected 15 D. brevis mites in the meibum of a 46-year-old male patient whose epilated eyelashes were negative5).
Indications: Refractory cases with posterior blepharitis or MGD-like findings but no Demodex detected in epilated eyelashes
In vivo confocal microscopy
Technique: Using a corneal confocal microscope, non-invasively visualize mites within eyelash follicles in vivo.
Advantages: Allows repeated observation, no need for removal
Challenges: Equipment availability and cost, standardization of evaluation are issues1)
Supplementary Tests (Combined Assessment with MGD)
For combined assessment with MGD, the following supplementary tests are used4).
Test
Purpose
Role
Meibography (infrared)
Evaluation of meibomian gland dropout, shortening, and dilation
Useful as a supplementary diagnostic tool4)
Tear break-up time (BUT)
Assessment of tear film lipid layer instability
Listed as an evaluation item4)
Fluorescein staining
Evaluation of corneal and conjunctival epithelial damage
Used to confirm ocular surface damage4)
Meibum expression (Shimazaki classification)
Obstructive findings item in MGD diagnostic criteria
Used to confirm obstructive changes4)
Interferometry
Quantitative evaluation of tear lipid layer
Auxiliary useful4)
The Japanese diagnostic criteria for hyposecretory MGD require all three of the following to be positive: subjective symptoms, periorificial findings (any of vascular dilation, mucocutaneous junction migration, or lid margin irregularity), obstructive findings (plugging), and Shimazaki classification grade 2 or higher4). Many cases of Demodex blepharitis also meet these MGD diagnostic criteria.
For treatment-resistant blepharitis, consider concurrent staphylococcal culture, eyelid biopsy, and Demodex detection1).
QHow are mites detected?
A
The basic method involves plucking about 4 eyelashes from each upper and lower lid and examining them under a light microscope for adult mites and larvae1)2). However, D. brevis may hide within the meibomian glands and may not be detected by this method1)5). In suspicious cases, after antiseptic treatment of the eyelid margin, the tarsal plate is compressed to express meibum, which is then directly observed under a microscope. In one report, 15 D. brevis mites were detected in the meibum of a 46-year-old male5). A non-invasive method, in vivo confocal microscopy, allows observation of mites within hair follicles in living tissue, but the availability and cost of the equipment are challenges1).
Demodex blepharitis follows a chronic course, and there is no strong evidence for a complete cure. Treatment goals are reduction of mite count, disappearance of cylindrical dandruff, improvement of symptoms, control of complications (MGD, BKC, RCE, chalazion), and long-term stabilization of the ocular surface1)4)6). The treatment strategy is based on basic eyelid care, with the addition of acaricidal agents in a layered approach.
Warm compresses, eyelid hygiene, and meibum expression are the foundation of treatment for MGD and blepharitis in general4).
Warm compresses: Use a commercially available warm eye mask, twice daily for at least 5 minutes. This raises the eyelid temperature to the melting point of meibomian gland lipids, promoting meibum liquefaction and secretion4).
Eyelid hygiene: Use a cotton ball moistened with water or a commercially available eyelid cleanser, and gently clean the eyelash roots with a cotton swab. While improvements in subjective symptoms, meibomian gland orifice findings, meibum grade, tear break-up time, and keratoconjunctival epithelial damage are expected, adverse events such as eye irritation may occur depending on the cleanser used4).
Meibum expression: Consider in cases with obstructive MGD. Use specialized instruments such as the Arita meibomian gland expression forceps, and perform regularly in the outpatient setting4).
Tea tree oil is an essential oil extracted from Melaleuca alternifolia, and its main component, terpinen-4-ol (T4O), exerts acaricidal effects7)8). The mechanism of action is thought to be mite nerve paralysis via acetylcholinesterase inhibition1)6).
50% TTO once-weekly clinic wiping + 10% TTO daily home wiping for one month has been reported to eliminate mites, reduce inflammation of the eyelid margin, conjunctiva, and cornea, decrease tear IL-1β and IL-17 levels, and improve ocular surface irritation symptoms6)7)10).
5% TTO ointment applied daily to the eyelids as home therapy also achieved a significant reduction in mite count and improvement in itching after 4 weeks6).
For the T4O single-agent formulation Cliradex®, a regimen of once daily for mild cases and twice daily for moderate to severe cases for an initial 2 months has been proposed6).
In an RCT using a tea tree oil-containing cleansing agent, improvements in subjective symptoms, meibomian gland orifice findings, meibum grade, BUT, and keratoconjunctival epithelial damage were demonstrated4). However, as an adverse event, ocular irritation was observed in 52.5% (21 of 40 cases) of the TTO-containing cleansing agent group, and when using it, adjustment of concentration and frequency and confirmation of history of skin hypersensitivity are important4).
Oral ivermectin: A regimen of 200 μg/kg administered twice on Day 0 and Day 7 is used9). In a study of 24 eyes of 12 patients with refractory posterior blepharitis, a significant decrease in D. folliculorum count, improvement in Schirmer I value, and improvement in BUT were reported9). It induces paralysis by acting on GABA receptors in mites1).
Topical ivermectin cream 1%: When combined with metronidazole, the miticidal and anti-inflammatory effects are enhanced1).
Metronidazole: It has both DNA damage via nitro radicals and anti-inflammatory effects, and is used orally or topically1).
0.25% povidone-iodine / DMSO formulation: A case report showed improvement in symptoms and findings of anterior and posterior Demodex blepharitis with twice-daily topical application11).
1.5% azithromycin hydrate ophthalmic solution: It may be used to improve subjective symptoms, meibomian gland orifice findings, and meibum grade4).
0.1% fluorometholone ophthalmic solution: Used short-term in combination for cases with severe inflammation. In Japan, it is covered by insurance only when complicated with blepharitis4).
Minocycline hydrochloride 100 mg/day oral: It may be used for anti-inflammatory and lipid-regulating effects4).
Mechanical and Physical Therapy
Microblepharoexfoliation (BlephEx): An in-office procedure that mechanically removes cylindrical scales, debris, and mites from the eyelid margin using a rotating microsponge 1). It is also expected to disrupt bacterial biofilms, and when combined with tea tree oil therapy, improvements in OSDI and mite counts have been reported 1).
Meibomian gland probing: Improves meibum outflow in Demodex blepharitis complicated by obstructive MGD6).
LipiFlow® thermal pulsation: A 12-minute procedure combining internal heating and external compression, reported to improve meibum secretion, TBUT, and subjective symptoms 6).
IPL (Intense Pulsed Light) therapy: Kills mites through the thermal effect of broadband light (rising to approximately 49°C in vitro). Reductions in meibomian gland vascular dilation, mite counts, and subjective symptom improvement have been reported 1). After confirming approval and insurance coverage in the country, the indication should be considered at a specialized facility 4).
MGD: Enhance warm compress, expression, and azithromycin eye drops4)
Evaporative dry eye: Artificial tears, sodium hyaluronate eye drops. Diquafosol sodium eye drops are not covered by insurance for MGD alone and are not typically used for MGD alone4)
Pediatric blepharokeratoconjunctivitis (BKC): Systemic antibiotics, eye ointment, and therapeutic contact lenses in combination. In pediatric cases reported by Lee et al., aggressive antiparasitic treatment and corneal treatment were necessary for severe keratitis2)
QWhat care can I do at home?
A
The basics are three steps: warm compress, eyelid massage, and eyelid hygiene4)6). Apply a clean towel or a commercially available warm eye mask to the eyelids for at least 5 minutes twice daily4). Then gently massage the upper and lower eyelids in a vertical direction to promote meibomian gland secretion. Finally, carefully clean the eyelash roots with a cotton ball moistened with water or a dedicated cleansing agent4). Preparations containing tea tree oil have been reported to be added about once a week, with attention to concentration7)10). Avoid excessive rubbing, and also pay attention to hygiene of cosmetics and eyelash extensions. Daily continuation even after the acute phase subsides is key to preventing recurrence.
The pathophysiology of Demodex blepharitis is organized through multiple pathways: mechanical mechanisms, immunological mechanisms, bacterial vector hypothesis, and overlap with MGD pathology1)4)6).
1. Mechanical Mechanisms
Demodex folliculorum aggregates in multiple numbers within eyelash follicles and feeds on basal keratinocytes1)6). This causes local cell damage and reactive hyperkeratosis, and the formed keratin accumulates at the base of the eyelashes along with mite feces and debris, forming cylindrical dandruff1). Chronic inflammation around the follicle contributes to eyelash loss, misdirection, and follicle destruction.
On the other hand, Demodex brevis parasitizes alone within the ducts of the meibomian glands and Zeis glands, physically obstructing the glandular lumen1)5)6). Histologically, granulomatous reactions, acinar atrophy, and qualitative and quantitative decreases in lipid secretion are observed, presenting with MGD-like clinical findings and chalazion-like changes5)6). In the case reported by Zhang and Liang, 15 D. brevis mites were detected in the meibum of a 46-year-old man who presented with obstruction of meibomian gland openings, telangiectasia, and superficial keratopathy, indicating that intraductal parasitism can occur even when external findings are subtle5).
2. Immunological mechanisms
Excretions, secretions, and dead bodies of Demodex induce a delayed-type hypersensitivity reaction in the host1). This reaction is particularly pronounced in patients with rosacea and is thought to explain the high comorbidity rate of ocular rosacea and Demodex blepharitis1).
In the tear cytokine profile, increases in IL-1β, IL-17, and MMP-9 have been reported, and these cytokines have been confirmed to decrease after tea tree oil treatment6). Upregulation of Toll-like receptor 2 (TLR2) has also been reported, suggesting amplification of inflammation via the innate immune pathway1).
3. Bacterial vector hypothesis
It has been suggested that bacteria adhering to the surface or digestive tract of Demodex may act as independent inflammatory triggers1)6). Candidate bacteria include Bacillus oleronius, Staphylococcus aureus, Acinetobacter baumannii, and Streptococcus pneumoniae, and the hypothesis is that host immune responses to these antigens exacerbate chronic inflammation of the ocular surface1). In patients with rosacea, serum reactivity to B. oleronius antigens has been reported to be significantly higher than in healthy individuals1).
The pathophysiology of hyposecretory MGD is primarily organized into two core mechanisms4): obstruction of meibomian gland openings due to hyperkeratinization of the ductal epithelium and abnormal differentiation, acinar atrophy, and decreased meibum quality due to changes in meibocytes4). Upstream factors include aging, sex hormones (androgens), bacterial infection, Demodex, inflammation/allergy, neural factors, vascular factors, medications, and incomplete blinking4).
Therefore, Demodex blepharitis is positioned to add physicochemical stress to the ducts and acini at the entry side of the MGD pathological cascade, promoting the progression of MGD. In clinical practice, Demodex blepharitis and MGD exacerbate each other, so it is a principle to treat both simultaneously4)6).
5. Association with Rosacea
In patients with cutaneous rosacea, Demodex density increases several times that of healthy individuals1). Rosacea treatments such as oral doxycycline and topical ivermectin can simultaneously improve Demodex density and ocular symptoms1). Therefore, when evaluating chronic, treatment-resistant Demodex blepharitis, it is useful to collaborate with a dermatologist to assess systemic rosacea.
Lotilaner is an isoxazoline antiparasitic agent that specifically inhibits GABA-gated chloride channels and glutamate-gated chloride channels in mites, inducing spastic paralysis and killing them1)3). Since these channels have low sensitivity in host mammals, it has a favorable safety profile3).
The Phase 3 pivotal trial Saturn-1 was a randomized, vehicle-controlled, double-blind study involving 421 patients with Demodex blepharitis. Treatment with Lotilaner ophthalmic solution 0.25% twice daily for 6 weeks achieved a cylindrical dandruff resolution rate of 56%, a mite eradication rate (0–1 mites per 4 lashes) of 51.8%, and an eyelid margin erythema resolution rate of 31.1%3). Tolerability was rated good at 90.7%, with side effects mainly mild, such as burning sensation and mild visual acuity reduction1)3). The subsequent Saturn-2 trial confirmed similar results1).
In July 2023, the US FDA approved Lotilaner ophthalmic solution 0.25% (brand name XDEMVY®, formerly TP-03) as the first approved drug for Demodex blepharitis1). Approval in Europe is expected around 20271). As of 2026, it is not yet approved in Japan, and the status of approval application and review by PMDA should be monitored1).
Czepińska-Myszura et al. stated in their review that “among the new treatments, only Lotilaner eye drops have demonstrated high efficacy in large-scale clinical trials, while IPL and microblepharoexfoliation have only been validated in limited patient groups”1).
BlephEx is an office-based procedure that uses a rotating microsponge to mechanically remove cylindrical scales, debris, mites, and bacterial biofilm from the eyelid margin1). Although significant improvements in OSDI and mite counts have been reported when combined with tea tree oil therapy, further research is needed to verify long-term efficacy and recurrence prevention1).
Novel Topical Essential Oils and Natural Ingredients
In vivo confocal microscopy (IVCM) allows non-invasive visualization of mites within hair follicles and enables repeated assessments1). If PCR-based molecular detection and automated image analysis are applied clinically in the future, standardized quantitative evaluation of Demodex will become possible.
In an analysis of 9 cases by Lee et al., pediatric cases aged 5, 13, and 14 years were included, all presenting with blepharokeratoconjunctivitis accompanied by corneal ulcers and neovascularization2). In children with recurrent keratitis, the involvement of Demodex should be actively suspected2).
Additionally, Zhang and Liang reported a 46-year-old male case in whom D. brevis was hidden only within the meibum without any external findings, demonstrating that direct observation of meibum after eyelid margin cleansing can aid diagnosis in refractory cases5).
QIs Lotilaner (XDEMVY) available in Japan?
A
As of 2026, Lotilaner ophthalmic solution 0.25% (XDEMVY®) has been approved by the US FDA, but it is not yet approved in Japan or Europe1)3). Approval in Europe is expected around 20271). The approval status in Japan will depend on future PMDA review. Currently, treatment mainly involves tea tree oil-containing preparations, ivermectin (oral and topical), metronidazole, and microblepharoexfoliation1)6).
Aleksandra Czępińska-Myszura, Małgorzata Maria Kozioł, Beata Rymgayłło-Jankowska. Pharmacotherapy of Demodex-Associated Blepharitis: Current Trends and Future Perspectives. Pharmacy. 2025;13(5):148. doi:10.3390/pharmacy13050148.
Lee YI, Seo M, Cho KJ. Demodex Blepharitis: An Analysis of Nine Patients. The Korean journal of parasitology. 2022;60(6):429-432. doi:10.3347/kjp.2022.60.6.429. PMID:36588421; PMCID:PMC9806504.
Yeu E, Wirta DL, Karpecki P, Baba SN, Holdbrook M; Saturn I Study Group. Lotilaner Ophthalmic Solution, 0.25%, for the Treatment of Demodex Blepharitis: Results of a Prospective, Randomized, Vehicle-Controlled, Double-Masked Pivotal Trial (Saturn-1). Cornea. 2023;42(4):435-443. doi:10.1097/ico.0000000000003097.
Zhang N, Liang L. Demodex in Meibum. Ophthalmology. 2024.
Saama Sabeti, Ahmad Kheirkhah, Jia Yin, Reza Dana. Management of meibomian gland dysfunction: a review. Survey of Ophthalmology. 2020;65(2):205-217. doi:10.1016/j.survophthal.2019.08.007.
Gao YY, Di Pascuale MA, Li W, Baradaran-Rafii A, Elizondo A, Kuo CL, et al. In vitro and in vivo killing of ocular Demodex by tea tree oil. The British journal of ophthalmology. 2005;89(11):1468-73. doi:10.1136/bjo.2005.072363. PMID:16234455; PMCID:PMC1772908.
Sean Tighe, Ying-Ying Gao, Scheffer C. G. Tseng. Terpinen-4-ol is the Most Active Ingredient of Tea Tree Oil to KillDemodexMites. Trans. Vis. Sci. Tech. 2013;2(7):2. doi:10.1167/tvst.2.7.2.
Holzchuh FG, Hida RY, Moscovici BK, Villa Albers MB, Santo RM, Kara-José N, et al. Clinical treatment of ocular Demodex folliculorum by systemic ivermectin. American journal of ophthalmology. 2011;151(6):1030-1034.e1. doi:10.1016/j.ajo.2010.11.024. PMID:21334593.
Koo H, Kim TH, Kim KW, Wee SW, Chun YS, Kim JC. Ocular surface discomfort and Demodex: effect of tea tree oil eyelid scrub in Demodex blepharitis. Journal of Korean medical science. 2012;27(12):1574-9. doi:10.3346/jkms.2012.27.12.1574. PMID:23255861; PMCID:PMC3524441.
Pelletier JS, Capriotti K, Stewart KS, Capriotti JA. Demodex Blepharitis Treated with a Novel Dilute Povidone-Iodine and DMSO System: A Case Report. Ophthalmology and therapy. 2017;6(2):361-366. doi:10.1007/s40123-017-0097-3. PMID:28643231; PMCID:PMC5693835.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.