Drug-Induced Maculopathy is a general term for conditions in which systemically or locally administered drugs directly or indirectly cause toxicity to the macula and retina.
The mechanism of toxicity and clinical pattern vary depending on the causative drug. The following classification is useful for conceptual organization.
Features: Degeneration and destruction of the retinal pigment epithelium (RPE). Presents with bull’s eye maculopathy. Long-term use, high doses, and kidney disease are major risk factors.
Vascular injury / direct toxicity type
Representative drugs: Mitomycin C (MMC), cefuroxime, aminoglycosides
Features: Vascular occlusion, outer layer disruption, and retinal ischemia due to accidental intraocular contamination. Caused by inadvertent injection of local drugs or migration into the suprachoroidal space.
Features: Diverse mechanisms including mitochondrial toxicity (DDI), hyperosmotic crystal deposition (GCV), ERBB receptor-mediated RPE dedifferentiation (neratinib), and crystalline retinopathy (tamoxifen).
Many cases are reversible upon discontinuation of the causative drug, but some result in permanent or progressive vision loss. Early stages may appear normal on ophthalmoscopy, making OCT and electrophysiological tests essential for diagnosis.
QWhich drugs cause drug-induced maculopathy?
A
A wide variety of drugs can cause it, including chloroquine derivatives, immune checkpoint inhibitors, antiviral drugs (ganciclovir, didanosine), anticancer agents (mitomycin C, neratinib, tamoxifen), and antibiotics (cefuroxime). Because the toxic mechanism, clinical presentation, and prognosis vary greatly depending on the causative drug, it is important to always consider the patient’s medication history during examination.
Mitomycin C (MMC): Inadvertent intravitreal injection during trabeculectomy causes outer layer (IS/OS/EZ) disruption and multiple regional vascular occlusions1). Migration into the suprachoroidal space can cause regional retinal damage3).
Immune checkpoint inhibitors (ICIs): After administration of nivolumab and ipilimumab, VKH-like pachychoroidal changes (choroidal thickness 505–510 μm), SRF, and BALAD have been reported2). OCT shows relatively preserved outer retinal structures, and response to immunosuppressive therapy is good.
High-dose intravitreal ganciclovir (GCV): Cases have been reported with full-thickness hyperreflective vertical bands, ellipsoid zone (EZ) disruption, and neurosensory detachment (NSD) 4). With repeated administration, even when ophthalmoscopic and OCT findings are normal, visual field defects and multifocal electroretinogram (mfERG) amplitude reduction accumulate chronically 6).
Cefuroxime (inadvertent intracameral injection): OCT shows subretinal fluid (SMD) and schisis-like changes in the outer nuclear layer (ONL) 7). Early anterior chamber washout and anti-inflammatory treatment may lead to a favorable outcome.
Didanosine (DDI): Presents as mid-peripheral pigmentary retinopathy, sparing the macula9). In patients with ABCA4 mutations, toxicity can be severe, leading to serious foveal damage 5).
Neratinib (TKI): Cases have been reported showing OCT findings similar to macular telangiectasia type 2 (MacTel type II), including an inner limiting membrane (ILM) draped appearance and cavitation 8).
QWhat subjective symptoms are associated with drug-induced maculopathy?
A
Symptoms may include decreased vision, metamorphopsia, color vision abnormalities, paracentral scotomas, photophobia, and night blindness. In early stages, subjective symptoms may be minimal, and the condition may be discovered incidentally on OCT or visual field testing. In didanosine toxicity, night blindness may precede other symptoms 9).
Chloroquine (CQ) and Hydroxychloroquine (HCQ): Long-term use over 5 years, high dose >5.0 mg/kg/day (HCQ), and kidney disease are risk factors. The incidence rate after 5 years of use is approximately 0.5%.
Immune checkpoint inhibitors (ICIs): The incidence of ocular complications is about 1%. Melanoma, female sex, and combination therapy with nivolumab plus ipilimumab are considered high risk 2).
Tyrosine kinase inhibitors (TKIs) and neratinib: Synergistic effects with docetaxel due to CYP3A4 inhibition may contribute to increased toxicity 8).
Didanosine (DDI): Mitochondrial toxicity due to inhibition of mitochondrial DNA polymerase gamma (pol-γ) is the main mechanism 9). It may progress even after discontinuation 5).
Ganciclovir (GCV): The safety range for intravitreal injection is 200–2000 μg/0.1 mL. Cumulative doses of 40 mg have been reported to increase the risk of damage 4). Even repeated doses of 3 mg/0.1 mL can lead to chronic retinal damage 6).
Mitomycin C (MMC): Accidental intravitreal injection of 0.4 mg/mL has been observed to cause Müller cell degeneration from day 2 in animal studies 1). Migration into the suprachoroidal space also results in widespread retinal toxicity 3).
Cefuroxime: Caused by accidental injection into the anterior chamber7). This is an iatrogenic injury due to drug mix-up during eye surgery.
Specific genetic mutations have been shown to increase the risk of drug-induced toxicity.
CRB1 mutation: Increases susceptibility to DDI toxicity 9).
ABCA4 mutation: Acts synergistically with DDI toxicity, causing severe macular degeneration5).
QHow often should I see an ophthalmologist while using HCQ?
A
Baseline examination is recommended at the start of treatment, followed by annual screening from the fifth year onward (AAO guidelines). Patients with renal impairment, high doses, or long-term use require earlier and more frequent examinations. For details, see “4. Diagnosis and Examination Methods”.
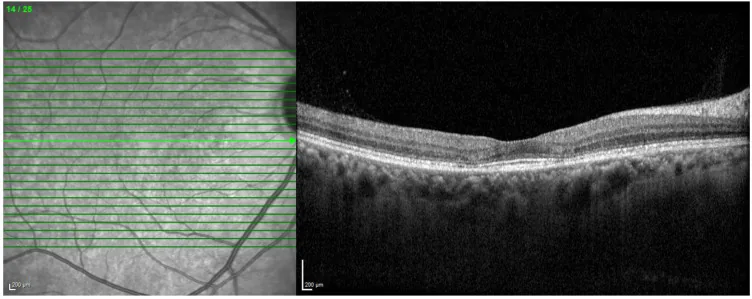
Kai Xiong Cheong; Charles Jit Teng Ong; Priya R Chandrasekaran; Jinzhi Zhao; Kelvin Yi Chong Teo; Ranjana Mathur. Review of Retinal Imaging Modalities for Hydroxychloroquine Retinopathy. Diagnostics (Basel). 2023 May 16; 13(10):1752. Figure 1. PMCID: PMC10217485. License: CC BY.
SD-OCT showing evident loss of the photoreceptors and outer retina in the parafoveal region, which causes the inner retinal layers to be displaced downwards around the fovea as the fovea is spared.
In the diagnosis of drug-induced maculopathy, it is important to identify the medications being taken and to combine multiple examination modalities.
SD-OCT
Indications: High-sensitivity detection of outer retinal structural changes. First-line for all drugs.
Findings: EZ disruption, outer retinal collapse, SRF, SMD, ONL changes1, 4, 7, 2). May appear normal in early stages.
Fundus Autofluorescence (FAF)
Indications: Noninvasive detection of RPE changes. Useful for CQ/HCQ and DDI.
Findings: Distribution of hypoautofluorescence (RPE atrophy) and hyperautofluorescence (RPE activation)3, 5).
Electroretinography and Visual Field
Indications: Quantitative assessment of functional impairment. Detects abnormalities earlier than morphological changes.
Findings: mfERG may be more sensitive than ffERG 7, 6). Humphrey 10-2 is useful for CQ/HCQ monitoring.
Fluorescein angiography (FA): Delineates areas of capillary nonperfusion. Useful for evaluating regional ischemia after inadvertent MMC injection 1, 3).
Genetic testing: Consider evaluation of CRB1, ABCA4, etc., when DDI toxicity is suspected 9).
Discontinuation of the causative drug is the most important and universally applicable first step. Discontinuation or change should be decided in close collaboration with the prescribing physician.
The basic treatment policy for each drug is shown below.
Causative drug
Main treatment
Prognosis
CQ/HCQ
Discontinuation and consideration of alternative drugs
Discontinue ipilimumab and start intravenous methylprednisolone 1 g/day. In reported cases, rapid improvement was seen within 2 days of administration, and resumption of nivolumab monotherapy was possible2).
There is a report that BCVA recovered to 0.02 logMAR (almost normal) after treatment with 22 mL BSS anterior chamber irrigation, topical steroids, NSAIDs, and subconjunctival injection of 40 mg depomedrol 7). Although the electroretinogram showed residual amplitude reduction after treatment, the visual prognosis was good 7).
High-dose intravitreal injection of ganciclovir (GCV)
There is a report that discontinuation of intravitreal injection and systemic administration of valganciclovir 900 mg/day led to improvement in OCT findings within one month 4).
Vitrectomy immediately after accidental intravitreal injection is considered, but many cases have poor prognosis 1, 3). Even in cases of migration into the suprachoroidal space, substantial recovery of visual function is limited 3).
QWill retinal damage recover if the drug is discontinued?
A
It varies greatly depending on the drug. For ICI-induced damage or inadvertent cefuroxime injection, good recovery can be expected with early appropriate treatment2, 7). On the other hand, damage caused by chloroquine derivatives or didanosine can progress even after discontinuation, requiring long-term follow-up5, 9).
Toxicity occurs through a cascade: binding to melanin → accumulation in lysosomes → pH elevation → lysosomal dysfunction → degeneration of RPE and photoreceptors.
It inhibits mitochondrial DNA polymerase gamma (pol-γ) and impairs mitochondrial DNA (mtDNA) synthesis. This disrupts energy metabolism in RPE and photoreceptors 5).
Lenis et al. (2022) reported a case in which a patient with CRB1 mutations showed markedly increased susceptibility to DDI toxicity and rapid progression of mid-peripheral pigmentary changes 9). CRB1 is a protein involved in maintaining the structure of the photoreceptor outer segment, and its loss of function is thought to lower the threshold for DDI toxicity.
Nunziata et al. (2026) reported a case of ABCA4-associated retinopathy superimposed with DDI toxicity 5). They suggested that the addition of DDI toxicity to pre-existing RPE vulnerability due to ABCA4 mutation resulted in much more severe and rapid macular damage than usual.
The main mechanism is cross-linking of DNA. In animal experiments, after intravitreal injection of 0.4 mg/mL, Müller cell degeneration was observed on day 2, RPE damage on day 4, and outer nuclear layer (ONL) degeneration on day 7 1). In migration into the suprachoroidal space, MMC reaches the retina regionally through the choroidal circulation, causing local vascular occlusion and outer layer collapse 3).
The proposed mechanism is: release of T cell immunosuppression → autoimmune reaction against ocular tissues (RPE, choroidal melanocytes, etc.) → VKH-like inflammation 2). Pachychoroidal changes, SRF, and BALAD are all considered findings reflecting immune-mediated damage to the choroid and RPE.
Overexpression of glutamate transporter 1 (GLT1) by cefuroxime is thought to reduce glutamate concentration around bipolar cells, leading to changes in electroretinogram findings7).
At high doses, osmotic damage due to crystal precipitation in the vitreous may injure photoreceptors4). With repeated low doses, chronic degeneration of photoreceptor outer segments is believed to cause functional impairment6).
A cascade of ERBB1/ERBB2 receptor tyrosine kinase inhibition → abnormal mTOR signaling → RPE dedifferentiation is hypothesized8). Morphological changes similar to MacTel type II may reflect disruption of the interaction between RPE and the internal limiting membrane.
QDoes genetic predisposition alter the risk of drug-induced retinal toxicity?
A
Can change. CRB1 mutations increase sensitivity to didanosine toxicity9), and ABCA4 mutations have been reported to cause synergistic macular damage with didanosine5). When using specific medications in patients with inherited retinal diseases, these risks should be evaluated and explained in advance.
7. Latest Research and Future Prospects (Research-stage Reports)
The relationship between DDI toxicity and CRB1/ABCA4 mutations suggests the potential for personalized medicine through genetic screening before drug use 9, 5). It is expected that a framework for predicting toxicity risk by conducting genetic testing before administering drugs to patients with inherited retinal diseases will develop in the future.
For patients using ICIs, a baseline ophthalmic examination before treatment and a system to detect changes early during the course are recommended 2). With the spread of new ICIs and ICI-TKI combination therapies, systematic accumulation of the frequency and patterns of ocular toxicity is required.
First Report of New TKI (Neratinib) Toxicity and Future Research
The MacTel type II-like toxicity caused by neratinib is the first report 8), suggesting that individual differences in CYP3A4 activity may influence toxicity risk. Predicting toxicity by measuring TKI-metabolizing enzyme activity will be a future research topic.
Elucidation of the Mechanism of MMC Suprachoroidal Migration
The migration of MMC into the suprachoroidal space was first reported in detail to cause regional retinal toxicity 3). Intraoperative drug management and intraocular pressure control may help prevent this, and further investigation is needed.
Reevaluation of the safety margin for high-dose GCV
Both severe retinal toxicity from a single high-dose GCV injection 4) and chronic damage from repeated low-dose administration 6) have been reported, making reevaluation of the safety margin for intravitreal GCV a challenge. Standardization of cumulative dose, injection interval, and monitoring methods is needed in the future.
Desai R, Jampol LM. RETINAL TOXICITY FOLLOWING PRESUMED INADVERTENT INTRAOCULAR INJECTION OF MITOMYCIN C DURING TRABECULECTOMY. Retinal cases & brief reports. 2023;17(3):329-333. doi:10.1097/ICB.0000000000001182. PMID:34293779; PMCID:PMC10121365.
Kilani A, Vounotrypidis E, König SF, Wolf A.. Retinal Toxicity after Initial Administration of Nivolumab and Ipilimumab. Case Rep Ophthalmol Med. 2023;2023:9931794. doi:10.1155/2023/9931794. PMID:38155755; PMCID:PMC10754639.
Nunziata A, Bianco L, Antropoli A, Arrigo A, Bandello F, Mansour AM, et al. ABCA4-associated retinopathy complicated by didanosine-associated retinal toxicity. American journal of ophthalmology case reports. 2026;41:102509. doi:10.1016/j.ajoc.2025.102509. PMID:41561667; PMCID:PMC12813201.
Hu F, Ma Y, Peng X. Suspected retinal toxicity after multiple intravitreal ganciclovir injections in a patient of CMV retinitis. Ocul Immunol Inflamm. 2024;32(5):525-528. doi:10.1080/09273948.2024.2316754. PMID: 38407965.
Ku JY, Wong SW, Steeples LR, Delaney C, Parry NRA, Fenerty C.. High dose cefuroxime causing retinal toxicity in a patient undergoing trabeculectomy. Am J Ophthalmol Case Rep. 2022;25:101343. doi:10.1016/j.ajoc.2022.101343. PMID:35198801; PMCID:PMC8841617.
Enghelberg M, Kaifee S. Suspected Neratinib Macular Toxicity Presenting As Macular Telangiectasia Type II. Cureus. 2023;15(1):e33964. doi:10.7759/cureus.33964. PMID:36824546; PMCID:PMC9941022.
Lenis TL, Botsford BW, Sarraf D, Papakostas TD. Didanosine-Associated Retinal Toxicity in a Patient With a Mutation in the CRB1 Gene. Journal of vitreoretinal diseases. 2022;6(4):329-331. doi:10.1177/24741264211044599. PMID:37007923; PMCID:PMC9976027.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.