Doyne Honeycomb Retinal Dystrophy (DHRD) is an autosomal dominant retinal dystrophy characterized by radial arrays of white drusen-like deposits in the posterior pole and around the optic disc. It is also known as Malattia Leventinese (MLVT) and familial dominant drusen. OMIM number is #126600. 1)
In 1899, British ophthalmologist Robert Doyne observed this finding in four sisters and first described it as a “honeycomb pattern.” In 1925, Vogt of Switzerland reported the same phenotype in the Leventine Valley and named it “Malattia Leventinese.” In 1999, Stone et al. identified the same mutation (R345W) in the EFEMP1 gene in both DHRD and MLVT families, proving they are the same disease.
The causative gene is EFEMP1 (EGF-containing fibulin-like extracellular matrix protein 1) located on chromosome 2p16.1, encoding the fibulin 3 protein. 2) This missense mutation Arg345Trp (R345W) causes abnormal deposits between Bruch’s membrane and the retinal pigment epithelium (RPE), leading to drusen formation. 1) It shares common pathological features with age-related macular degeneration, including drusen, Bruch’s membrane thickening, RPE atrophy, and complement activation. 1)
QHow is DHRD different from age-related macular degeneration?
A
Age-related macular degeneration is a multifactorial disease primarily caused by aging and occurs in older adults. In contrast, DHRD is caused by a single gene mutation (R345W in EFEMP1), with symptoms appearing in young to middle-aged individuals (40s-50s) and following an autosomal dominant inheritance pattern with family history. The distribution of drusen is characteristic, with radial arrays in the posterior pole and around the optic disc. Because both share common pathological pathways of drusen formation, Bruch’s membrane changes, and RPE atrophy, DHRD is also noted as a research model for age-related macular degeneration.
Drusen at the posterior pole and around the optic disc: Early-onset drusen along the vascular arcades. Radial arrangement is characteristic. 1)
Two types of drusen morphology: Two types are observed: large round drusen and small radial drusen. 2)
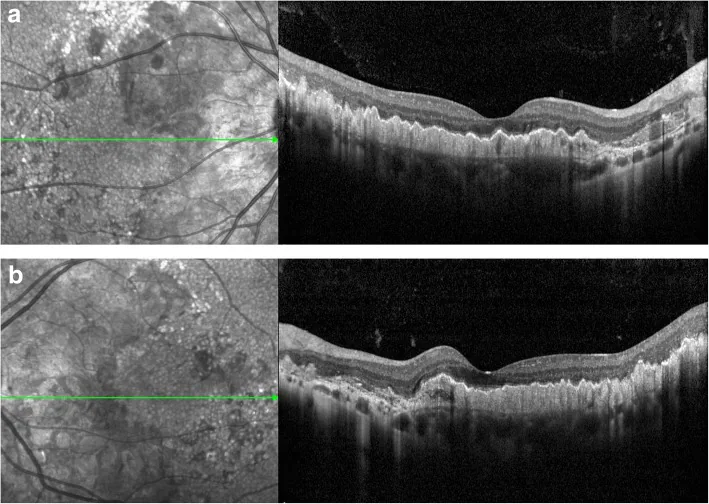
OCT findings: Diffuse changes in the RPE/Bruch’s membrane complex are shown. The neurosensory layer is relatively preserved. Drusenoid PED and double-layer sign are confirmed. 1)2)
Advanced stage findings
Drusen fusion and pigment changes: Drusen fuse, and pigment abnormalities occur in the RPE. 2)
RPE atrophy and scarring: May progress to central geographic atrophy. 2)
CNVM complication: Rare but a major cause of vision loss. May present with fibrovascular PED. 2)
Reduced electroretinogram amplitude: Reduced amplitude is confirmed on full-field electroretinography. 1)
Evaluation using multimodal imaging is useful for diagnosis and follow-up. 2)Fundus autofluorescence (FAF) shows hyperautofluorescence in drusen areas and hypoautofluorescence in areas of RPE atrophy. 2) Flicker threshold testing (FDT) detects reduced visual field sensitivity. 1)
QIs there individual variation in symptom severity?
A
Even within the same family, there are differences in severity. In some cases, good visual acuity is maintained until advanced stages, while in cases complicated by CNVM, rapid vision loss may occur. Regular fundus examinations are important for early detection of CNVM.
DHRD is an autosomal dominant disorder caused by a single gene mutation. Genetic information is shown below.
An overview of genetic information is provided below.
Item
Details
Causative gene
EFEMP1 (2p16.1)
Mutation
Exon 10, R345W
Inheritance pattern
Autosomal dominant
Encoded protein
Fibulin 3
EFEMP1 encodes EGF-containing fibulin-like extracellular matrix protein 1, which functions as an extracellular matrix component of Bruch’s membrane. The R345W mutation causes abnormal protein folding, leading to accumulation of basal laminar deposits between the RPE and Bruch’s membrane. 1) Additionally, EFEMP1 mutation is thought to inhibit CES1, which is involved in cholesterol efflux through suppression of EGFR signaling, thereby promoting lipid accumulation. Enhanced complement activation is also observed in mouse models of age-related macular degeneration and DHRD. 1)
The diagnosis of DHRD begins with recognition of young onset, family history, and characteristic drusen distribution patterns. 2) A combination of multimodal imaging evaluation and genetic testing is useful for definitive diagnosis. 2)
Pattern recognition: Young age (40s–50s) onset, bilateral symmetry, and radial drusen distribution around the posterior pole and optic disc are diagnostic clues. 2)
OCT: Evaluate RPE/Bruch’s membrane complex changes, drusenoid PED, double-layer sign, and preservation of the neurosensory layer. 2)
Fundus autofluorescence (FAF): Assess hyperautofluorescence of drusen and hypoautofluorescence pattern in areas of RPE atrophy. 2)
Genetic testing: Confirm EFEMP1 mutation by next-generation sequencing using NextSeq 550 (Illumina) with coverage ≥20×. According to ACMG guidelines, c.1033C>T (R345W) is classified as a pathogenic variant (PM2, PP3, PP5 criteria). 1)
QIs genetic testing always necessary for a definitive diagnosis?
A
If clinical findings are typical (young onset, bilateral symmetric posterior pole drusen, family history), a clinical diagnosis is possible without genetic testing. However, for definitive diagnosis, family screening, and genetic counseling, confirmation of the EFEMP1 R345W mutation is recommended.
Intravitreal anti-VEGF injection is a treatment option for cases with CNVM. Intravitreal injection of ranibizumab (0.5 mg) is used, and improvement in visual acuity and resolution of serous retinal detachment (SRF) have been reported after injection. 2)
Parameswarappa and Rani reported a 44-year-old woman (DHRD) who developed type 1 choroidal neovascular membrane, and after a single injection of ranibizumab, BCVA improved from 20/40 to 20/30, with resolution of SRF. 2) There are also reports of CNVM treatment with photodynamic therapy (PDT/verteporfin). 2)
QCan nanosecond laser (2RT) treatment be received?
A
2RT (nanosecond pulse laser) has been reported to improve function in case reports as a new treatment for DHRD, but it is currently an investigational treatment and has not been established as standard therapy. For details, see “Latest Research and Future Prospects” section.
EFEMP1 (EGF-containing fibulin-like extracellular matrix protein 1) functions as an extracellular matrix component of Bruch’s membrane. 1) The R345W mutation causes abnormal protein folding, leading to accumulation of basal laminar deposits between the RPE and Bruch’s membrane. 1) These deposits form the basis of drusen formation.
Drusen formation: abnormal deposition of material on Bruch’s membrane
Bruch’s membrane thickening: decreased permeability due to structural changes
RPE atrophy: degeneration of the retinal pigment epithelium due to nutritional deficiency
Complement activation: complement system upregulation has been confirmed in mouse models of both diseases
Regarding the impact on EGFR signaling, the EFEMP1 R345W mutation excessively suppresses the EGFR pathway and reduces expression of CES1, which is involved in cholesterol efflux. This promotes lipid accumulation and is thought to lead to drusen formation.
Electrophysiological studies show reduced amplitude in full-field electroretinography, suggesting dysfunction of both rods and cones. 1)FDT perimetry reveals a significant decrease in visual field sensitivity. 1)
QWhy is DHRD useful for age-related macular degeneration research?
A
DHRD shares the same molecular and pathological pathways as age-related macular degeneration (Bruch’s membrane changes, RPE atrophy, complement activation) but is caused by a single gene mutation (R345W), allowing clear analysis of causal relationships. While age-related macular degeneration is a multifactorial disease involving genomic and environmental factors, making mechanistic analysis difficult, the DHRD model provides a suitable system for studying these common mechanisms.
7. Latest Research and Future Perspectives (Research Stage Reports)
2RT (2-minute Retina Treatment) is a non-invasive treatment using ultra-low energy nanosecond pulse laser (400μm spot, 3 nanoseconds, 532nm, 0.15-0.45mJ). It is hypothesized to promote RPE debridement and layer reformation through wound healing response. 1)
Cusumano et al. (2023) reported 2RT treatment in 3 DHRD patients (aged 41-46) with up to 30 months of follow-up. 1) Main results were as follows:
Visual acuity: Case 1 showed improvement of 2-10 letters
FDT visual field sensitivity: Case 2 showed improvement from OD MD −12dB, Case 3 from OS MD −9dB
Full-field ERG amplitude: Significant increase confirmed in Cases 1 and 2
Safety: No treatment-related adverse events (though cystoid macular edema appeared at 24 months in Case 1)
Additionally, rod-specific ERG improvement (full-field ERG improvement, no multifocal ERG change) was observed, suggesting a mechanism primarily targeting the rod system. 1) Furthermore, functional improvement was seen in untreated fellow eyes in some cases, suggesting possible systemic indirect induction effects. 1)
This report is limited to a case series (3 cases) evidence level; large-scale RCTs have not been conducted. Establishing the efficacy and optimal protocol for repeated laser sessions remains a future challenge. 1)
Cusumano A, Falsini B, D’Ambrosio M, et al. Long-term structural and functional assessment of Doyne honeycomb retinal dystrophy following nanosecond 2RT laser treatment: a case series. Case Rep Ophthalmol. 2023;14:626-639.
Parameswarappa DC, Rani PK. Utility of pattern recognition and multimodal imaging in the diagnosis and management of doyne honeycomb retinal dystrophy complicated with type one choroidal neovascular membrane. BMJ Case Rep. 2021;14:e237635.
Tsang SH, Sharma T. Doyne Honeycomb Retinal Dystrophy (Malattia Leventinese, Autosomal Dominant Drusen). Adv Exp Med Biol. 2018;1085:97-102. PMID: 30578491.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.