Acute Exudative Polymorphous Vitelliform Maculopathy (AEPVM) is a rare retinal disease characterized by bilateral, multiple yellowish-white subretinal lesions corresponding to serous retinal detachment. It was first reported by Gass et al. in 1988 (Trans Am Ophthalmol Soc 1988).
Age of onset ranges from 13 to 69 years, with no gender predilection. 1) It occurs mainly in Caucasians but has also been reported in other races. Only about 20 idiopathic cases have been reported in the literature. 1)
AEPVM is classified into the following two types based on etiology:
Idiopathic: thought to involve viral infection or autoimmune mechanisms
Paraneoplastic: caused by malignant tumors or immune checkpoint inhibitors
This disease is classified under ICD-10 code H35.89 (Other specified retinal disorders).
QHow rare is AEPVM?
A
Only about 20 idiopathic AEPVM cases have been reported in the literature, making it an extremely rare disease. 1) Including paraneoplastic cases, the number of reports is increasing, but both types have few cases worldwide.
The main fundus finding is bilateral, symmetric, multiple yellowish-white subretinal lesions. The morphology of the lesions is diverse, taking various forms such as round, oval, or curvilinear. They are mainly located in the macula, but bleb-like lesions may also be observed along the vascular arcades. 1)
The yolk-like material within the lesions may settle downward due to gravity, forming a meniscus-like fluid level (pseudohypopyon). 1) There is no vitreous inflammation or vasculitis, and no optic disc abnormalities. 1)
Fundus findings differ between the acute and recovery phases. The findings for the two stages are shown below.
A comparison between the acute and recovery phases is shown below.
AEPVM is classified into two types: idiopathic and paraneoplastic, each with different causes and pathogenesis.
Idiopathic
Prior infection history: Viral prodromes (HCV, Coxsackie B, EBV, HIV, COVID-19), syphilis, Lyme disease, and other infections may precede onset.
Ocular trauma: Ocular trauma before onset has been reported as a trigger in some cases.
Autoimmune hypothesis: Anti-peroxiredoxin 3 (PRDX3) antibodies are detected in the acute phase and disappear after remission. Autoantibodies against RPE and photoreceptor proteins are thought to be involved in the pathogenesis.
Idiopathic cases: There are also purely idiopathic cases where systemic and genetic tests are all negative. 1)
Paraneoplastic
Melanoma: Cutaneous melanoma and choroidal melanoma are the most common causative malignancies.
Other malignancies: Associations with lung cancer, breast cancer, colon cancer, etc., have been reported.
Immune checkpoint inhibitors: May occur in association with the use of BRAF inhibitors (vemurafenib, dabrafenib) and PD-1 inhibitors (pembrolizumab, nivolumab).
Pathogenesis: It is thought that cross-reactivity (molecular mimicry) between tumor antigens and retinal antigens triggers an autoimmune response against RPE and photoreceptors.
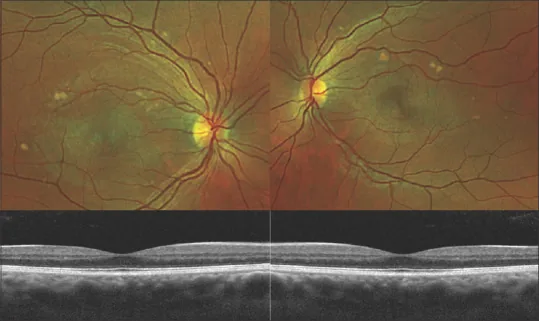
Torres-Costa S, Penas S, Carneiro Â, et al. Idiopathic Acute Exudative Polymorphous Vitelliform Maculopathy: Insight into Imaging Features and Outcomes. Case Rep Ophthalmol Med. 2020;2020:7254038. Figure 1 and Figure 2. PMID: 32082665; PMCID: PMC7008265. DOI: 10.1155/2020/7254038. License: CC BY 4.0.
A side-by-side view of fundus photographs and OCT of both eyes. The distribution of macular lesions and subretinal changes are summarized for easy understanding.
The diagnosis of AEPVM is one of exclusion, requiring a systematic process to rule out similar diseases. A combination of multimodal imaging is key to diagnosis. 1)
Imaging Tests
OCT (Optical Coherence Tomography): Detects dome-shaped neurosensory retinal detachment and hyperreflective or isoreflective subretinal deposits. During the recovery phase, resolution of subretinal fluid and reattachment of the RPE can be observed. Thickening of the ellipsoid zone is also noted. 1)
FAF (Fundus Autofluorescence): The vitelliform material shows hyperautofluorescence. This is the most important test for diagnosis. 1) It reflects accumulation of lipofuscin and fluorescent pigments.
FA (Fluorescein Angiography): The vitelliform material appears hypofluorescent or non-fluorescent. It characteristically shows a pattern inverted from FAF. No leakage is observed.
Functional and Genetic Tests
EOG (Electrooculography): A decreased Arden ratio is observed, reflecting RPE dysfunction.
Genetic Testing: Searching for BEST1 and PRPH2 mutations using next-generation sequencing panels is important. Negative results for these mutations can rule out Best vitelliform macular dystrophy. 1)
Systemic Examination: A thorough systemic workup to rule out malignancy is mandatory. 1)
AEPVM must be differentiated from the following diseases.
Best vitelliform macular dystrophy (BVMD): Differentiated by genetic testing (BEST1 mutation). AEPVM does not have BEST1 mutations. 1)
Adult-onset foveomacular vitelliform dystrophy (AVMD): Differentiated by the presence or absence of PRPH2 mutations.
Vogt-Koyanagi-Harada disease (VKH): FA shows marked hyperfluorescence of the optic disc and pin-point leakage. AEPVM can be differentiated by the absence of leakage.
QHow to differentiate from Best disease (Best vitelliform macular dystrophy)?
A
Best disease is a hereditary disorder caused by mutations in the BEST1 gene and can be differentiated by genetic testing. In AEPVM, next-generation sequencing genetic testing shows negative for BEST1 and PRPH2 mutations. 1) The onset pattern (acute vs. gradual) and family history also aid in differentiation.
There is no established drug therapy for AEPVM. Idiopathic AEPVM is a self-limiting disease, and spontaneous recovery can be expected.
Observation is the mainstay: Regular fundus examination and OCT monitoring are performed. In the report by Fernandes et al., complete remission was achieved after 6 months. 1)
Steroid therapy: Its efficacy for idiopathic AEPVM has not been confirmed and is not recommended as standard treatment at present.
Paraneoplastic AEPVM: If association with immune checkpoint inhibitors (BRAF inhibitors, PD-1 inhibitors) is suspected, the appropriateness of drug discontinuation should be determined in collaboration with oncology, considering the treatment status of the primary tumor. Switching to alternative immunotherapy may also be considered.
QWhat is the visual prognosis for idiopathic AEPVM?
A
Idiopathic AEPVM is a self-limiting disease, and spontaneous visual recovery is expected in many cases. In the case by Fernandes et al., best-corrected visual acuity improved to 20/25 in both eyes after 6 months, and OCT confirmed complete resolution of subretinal fluid. 1) However, the degree of recovery varies by case.
Dysfunction of the retinal pigment epithelium (RPE) leads to lipofuscin accumulation and serous retinal detachment. Physical separation of the neurosensory retina and RPE impairs normal phagocytosis of photoreceptor outer segments. Shed photoreceptor outer segments are thought to accumulate in the outer retina and subretinal space (Spaide hypothesis). The hyperautofluorescence observed on FAF reflects this accumulation of lipofuscin and fluorescent pigments.
Autoantibodies against RPE and photoreceptor proteins are thought to be involved in the pathogenesis. The following have been reported as putative target antigens of autoantibodies:
Recoverin
Transducin-α
Peroxiredoxin 3 (PRDX3): Anti-PRDX3 antibodies have been detected in the acute phase of idiopathic AEPVM and disappeared after remission in reported cases.
Carbonic anhydrase 2
120 kDa photoreceptor protein
145 kDa interphotoreceptor retinoid-binding protein
In paraneoplastic cases, cross-immune reactions (molecular mimicry) between tumor antigens and common antigens of the retina and RPE are speculated to cause the formation of vitelliform lesions.
7. Latest Research and Future Perspectives (Reports at Research Stage)
The combination of color fundus photography, SD-OCT, and FAF is making it possible to clinically diagnose AEPVM without invasive testing. 1) Each modality provides complementary information, and the inversion pattern of FAF and FA is key to diagnosis.
The use of next-generation sequencing panels allows comprehensive detection of genetic mutations such as BEST1 and PRPH2. Standardization of genetic testing contributes to improved accuracy of exclusion diagnosis. 1)
New challenges in the era of immune checkpoint inhibitors
With the widespread use of BRAF inhibitors (vemurafenib, dabrafenib) and PD-1 inhibitors (pembrolizumab, nivolumab), the association between these drugs and paraneoplastic AEPVM has emerged as a new clinical challenge. As immunotherapy becomes more common, the number of reported cases of paraneoplastic AEPVM may increase.
Need for case accumulation and large-scale studies
Only about 20 cases of idiopathic AEPVM have been reported in the literature. 1) To elucidate the etiology and develop treatments, multicenter case accumulation and large-scale prospective studies are necessary.
Fernandes et al. (2023) reported a case of idiopathic AEPVM in a man in his 60s, in which systemic examination and genetic testing using a next-generation sequencing panel were both negative. After 6 months, best-corrected visual acuity improved to 20/25 in both eyes, and SD-OCT confirmed complete resolution of subretinal fluid. 1)
Joana Silva Fernandes, Pedro Prata Gomes, Pedro Neves, João Pedro Marques. Idiopathic acute exudative polymorphous vitelliform maculopathy: the importance of multimodal imaging, systemic workup and genetic testing. BMJ Case Rep. 2023;16(6):e253969. doi:10.1136/bcr-2022-253969.
Osman M, Mehana O, Eissa M, Zeineldin S, Sinha A. Coronavirus Disease 2019-induced Acute Exudative Polymorphous Vitelliform Maculopathy. Middle East Afr J Ophthalmol. 2022;29(4):235-237. PMID: 38162565.
Lentzsch AM, Dooling V, Wegner I, Di Cristanziano V, Sadda SR, Freund KB, et al. ACUTE EXUDATIVE POLYMORPHOUS VITELLIFORM MACULOPATHY ASSOCIATED WITH PRIMARY EPSTEIN-BARR VIRUS INFECTION. Retin Cases Brief Rep. 2022;16(6):740-746. PMID: 33031214.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.