Chemical
Onset: Within 24 hours after birth
Findings: Only mild redness and tearing
Course: Resolves spontaneously in 2–4 days

Neonatal conjunctivitis (ophthalmia neonatorum) is inflammation of the conjunctiva occurring within 28 to 30 days after birth. Historically, in 1880, Crede introduced 1% silver nitrate eye drops, which greatly contributed to the prevention of gonococcal conjunctivitis. Currently, prophylaxis with antibacterial eye drops is the standard.
The global incidence is 2.04% (95% CI 0.70–5.79%), and the prevalence is 7.79% (95% CI 2.93–19.10%). 1) There is significant regional variation, with rates of 6.90% in low-income countries and 1.36% in high-income countries. 1) It is estimated that approximately 10,000 cases occur worldwide each year. 1)
The mode of delivery and gestational age also affect the incidence rate.
Etiology is broadly classified into chemical, bacterial, and viral causes. Among bacterial causes, chlamydia is the most frequent, while gonococcus leads to the most severe outcomes.
The global incidence is approximately 2.04%, with an estimated 10,000 cases per year. 1) There are regional differences: 1.36% in developed countries, while it reaches 6.90% in low-income countries.
Newborns cannot express symptoms. Parents or medical staff must observe objectively.
In newborns, there is decreased tear secretion, lack of secretory IgA, and reduced lysozyme activity, making them vulnerable to infection.
The timing of onset is the most important clue for determining the cause. Characteristic findings for each cause are shown below.
Chemical
Onset: Within 24 hours after birth
Findings: Only mild redness and tearing
Course: Resolves spontaneously in 2–4 days
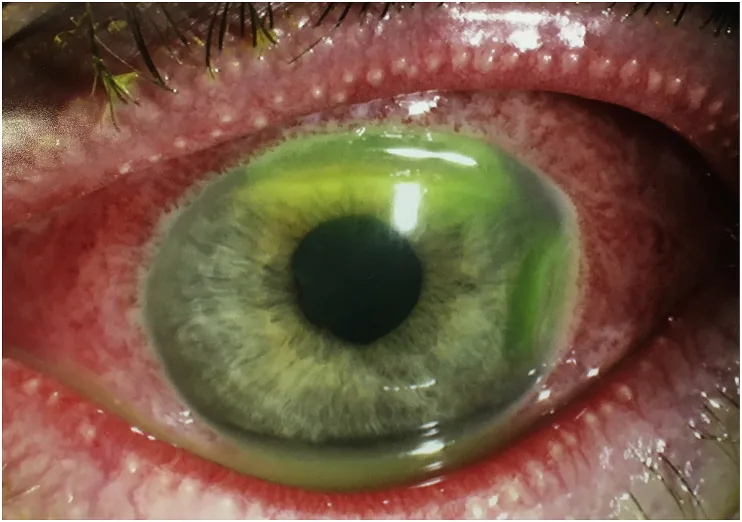
Gonococcal
Onset: 1–3 days after birth
Findings: Profuse purulent discharge (gonococcal ophthalmia neonatorum), severe eyelid swelling
Characteristic: The only bacterium capable of adhering to and invading healthy corneal epithelium. Risk of corneal ulcer → perforation → endophthalmitis.
Chlamydial
Onset: 3–10 days after birth
Findings: Pseudomembranous conjunctivitis (no follicle formation), velvety hyperemia of the palpebral conjunctiva, bloody discharge
Complications: Nasopharyngitis and pneumonia occur in 10–20% of cases
Viral (HSV)
Onset: 1–2 weeks after birth
Findings: Fine dendritic or geographic corneal ulcers (newborns may lack characteristic findings)
Caution: Neonatal herpes simplex virus infection can progress to systemic infection
Moraxella species develop after 7–10 days of life and are called pseudogonococcal conjunctivitis.
The time of onset is the most important clue for estimating the cause. Chemical conjunctivitis typically occurs within 24 hours, gonococcal at 1–3 days, chlamydial at 3–10 days, and herpes simplex virus at 1–2 weeks after birth. However, microbiological testing is necessary for a definitive diagnosis.
The most common route of infection is through the birth canal. Maternal sexually transmitted infections are the main risk factors.
Other risk factors include the following:
Prophylactic eye drops, starting with the Credé method (1% silver nitrate), are effective. A Cochrane review of 30 trials involving 79,198 newborns showed that the use of prophylactic agents reduces the incidence of all-cause conjunctivitis (moderate certainty). 2)
The five prophylactic agents recommended by the WHO are as follows: 2)
Even with cesarean section, the incidence is reported to be 1.88%, so it cannot be completely prevented. 1) Because routes other than birth canal infection (such as ascending infection) may be responsible, caution is necessary even after cesarean section.
Differentiation based on the time of onset is most important; refer to the “Clinical Findings” section to estimate the cause. Microbiological testing is essential for a definitive diagnosis.
The combination of onset timing and staining findings is key to diagnosis.
| Staining method | Target | Findings observed |
|---|---|---|
| Gram stain | Gonococcus | Gram-negative diplococci phagocytized by neutrophils |
| Giemsa stain | Chlamydia | Inclusion bodies (Prowazek bodies) |
| Fluorescein staining | Corneal lesions | Check for epithelial defects under cobalt blue light |
It is important to exclude diseases with similar symptoms.
Treatment is selected according to the cause. We focus on treatments in Japan and also supplement with standard protocols overseas.
The following is the treatment protocol in Japan.
| Cause | Recommended Treatment |
|---|---|
| Chemical | Artificial tears QID (wait for spontaneous resolution) |
| Gonococcal | Ceftriaxone 25–50 mg/kg single dose |
| Chlamydial | Azithromycin 20 mg/kg for 3 days4) |
| Herpes simplex virus | Acyclovir IV 45 mg/kg/day for 14–21 days |
Oral erythromycin is effective as systemic treatment for chlamydial conjunctivitis, but caution is needed regarding its association with infantile hypertrophic pyloric stenosis (IHPS).
In neonates, the use of ceftriaxone carries a risk of hyperbilirubinemia. 3) Therefore, in severe cases complicated by orbital cellulitis, the use of cefotaxime is recommended. When administering, it is important to select the drug after confirming the neonate’s jaundice status.
The neonatal eye is more vulnerable to infection compared to adults. The main factors are as follows:
Pseudomembrane is fibrin, neutrophils, and inflammatory exudate attached to the conjunctiva. In chlamydial conjunctivitis, follicles do not form due to underdeveloped adenoid tissue (pseudomembranous conjunctivitis).
Gonococcus is the only bacterium that can infect even eyes with healthy corneal epithelium. Its pathogenicity is due to the following mechanisms.
In Kenya, corneal lesions have been reported in up to 16% of affected children, 2) and early treatment is essential.
Chlamydia (Chlamydia trachomatis) is an obligate intracellular parasite. Outside cells, it exists as the infectious elementary body (EB), and inside cells it transforms into the replicative reticulate body (RB). It forms inclusion bodies (Prowazek bodies) within infected epithelial cells. Adult inclusion conjunctivitis is characterized by many large, solid follicles in the lower conjunctival fornix, whereas neonatal inclusion conjunctivitis typically develops around 7 days after birth and lacks follicles due to underdeveloped lymphoid tissue.
In addition to the traditional major pathogens, reports of new pathogens are accumulating.
Mechel et al. (2021) reported the first case of neonatal conjunctivitis due to SARS-CoV-2 in a 4-day-old girl. 7) She presented with subconjunctival hemorrhage and mucopurulent discharge, which resolved spontaneously within 8 days.
Albuquerque et al. (2024) reported that Neisseria meningitidis accounts for 1–2% of neonatal conjunctivitis cases, with a 10–29% risk of progression to invasive disease. 5) Complete recovery was achieved with intravenous cefotaxime 200 mg/kg/day for 7 days.
Merzouk et al. (2025) reported that enteric gram-negative rods (e.g., E. coli) are increasing in NICU-associated infections. The maternal E. coli colonization rate was 19.9%, and the vertical transmission rate was 21.4%. 8)
Das (2023) reported that in a Korean study, Acinetobacter baumannii accounted for 1.2% of neonatal conjunctivitis cases, while S. aureus accounted for 52.4%. 6) Multidrug-resistant A. baumannii has become a problem as a cause of NICU-associated nosocomial infections.
A Cochrane review (Malik and Gilbert 2022) concluded that no superiority among prophylactic agents has been established to date, and the selection of the optimal prophylactic agent remains a topic for future research. 2)
Law et al. (2024) reported two cases of neonatal conjunctivitis that progressed to orbital cellulitis due to treatment delay. 3) This again highlights the importance of early diagnosis and treatment intervention.
Asiamah R, Owusu G, Amoako PT, Amponsah R, Adator E, Kyei S. Epidemiology of ophthalmia neonatorum: a systematic review and meta-analysis. BMC pediatrics. 2025;25(1):31. doi:10.1186/s12887-024-05382-x. PMID:39810179; PMCID:PMC11730469.
Malik ANJ, Gilbert C. Cochrane corner: interventions for preventing ophthalmia neonatorum. Eye (London, England). 2022;36(2):356-357. doi:10.1038/s41433-021-01803-8. PMID:34642498; PMCID:PMC8807712.
Law NL, Tan VC, Lim TH, Nurul Rosli A. Ophthalmia neonatorum complicated with neonatal orbital cellulitis: A case series. Malaysian family physician : the official journal of the Academy of Family Physicians of Malaysia. 2024;19:5. doi:10.51866/cr.438. PMID:38371721; PMCID:PMC10866719.
Nwokeji I, Ding K, Ketner S. A Case of Neonatal Chlamydial Conjunctivitis: Illustrating the Typical Aspects of Presentation and the Importance of Empiric Treatment and a Multidisciplinary Approach. Cureus. 2024;16(7):e64463. doi:10.7759/cureus.64463.
Albuquerque C, Dias ME, Pelicano M, Banganho D, Morais RB. Neisseria meningitidis: The Unforeseen Agent of Acute Neonatal Conjunctivitis. Cureus. 2024;16(7):e65681. doi:10.7759/cureus.65681. PMID:39205736; PMCID:PMC11357735.
Das G. Acinetobacter baumannii ophthalmia neonatorum - A very rare presentation. Indian journal of ophthalmology. 2023;71(6):2595-2597. doi:10.4103/ijo.IJO_2240_22. PMID:37322687; PMCID:PMC10417955.
Mechel E, Trinh M, Kodsi S, Hymowitz M, Kainth MK, Lee AM.. Ophthalmia neonatorum as the presenting sign of SARS-CoV-2. J AAPOS. 2021;25(4):230-231. doi:10.1016/j.jaapos.2021.03.001. PMID:33774164; PMCID:PMC7989099.
Merzouk B, Schwartzman K, Yossuck P, Gunasekaran V. A Rare Case of Neonatal Escherichia coli Conjunctivitis With Maternal Asymptomatic Bacteriuria. Cureus. 2025;17(9):e92936. doi:10.7759/cureus.92936. PMID:41141014; PMCID:PMC12547613.