Eye movement examination is a series of tests that assess the range of eye movement, eye position, and whether diplopia is present. The main tests are the following three.
Assessment of version and duction by visual inspection: assess conjugate movements of both eyes in the same direction (version) and movements of one eye alone (duction) by visual inspection
Hess chart (Hess red-green test): use red-green glasses to record the site and degree of eye movement disorder
Fixation field test: record the range of diplopia using the monocular fixation field and binocular single vision field
The significance of the Hess chart and fixation field test is to record the degree of ocular motility disorder and diplopia. It is rare for these tests to detect abnormalities for the first time or to be useful for making a definitive diagnosis. Performing the eye movement examination by visual inspection while confirming the patient’s perception of diplopia provides far more information.
It is indicated for patients with diplopia, restricted eye movement, or abnormal head posture (compensatory head posture). In addition to evaluating paralytic strabismus such as abducens, oculomotor, and trochlear nerve palsies, and mechanical restriction due to thyroid eye disease or orbital floor fracture, it is also used to objectively record pre- and postoperative changes in strabismus surgery. The Hess chart and gaze field test are mainly for “recording,” and should basically be performed together with visual inspection of eye movements.
2. Prerequisite for the examination: observation of compensatory head posture
Do not focus only on the eyes; first observe the patient as a whole and check for any postural abnormalities. Head posture abnormalities (compensatory head posture) are evaluated in three rotational directions: face turn to either left or right (horizontal plane), chin up and chin down (sagittal plane), and head tilt to either left or right (coronal plane).
Compensatory head posture is a natural adaptation to correct ocular motility disorders and strabismus, and its direction can help infer the affected muscle and the direction of the deficit.
Vertical and torsional strabismus such as superior oblique palsy
After confirming the compensatory head posture, proceed to visual inspection of version and duction in nine directions.
QWhat should be done first for a patient complaining of diplopia?
A
First observe the patient as a whole and check for compensatory head posture (face turn, chin-up, head tilt). Next, visually assess eye movements in nine directions and confirm any movement limitation and the direction in which diplopia appears in each gaze direction. After that, perform Hess chart testing and gaze field testing for record keeping. Because the priority of the differential diagnosis changes depending on whether the diplopia is horizontal or vertical, the most important first step is to determine the direction of the diplopia and the direction of ocular movement limitation by visual inspection.
3. Principles and procedures of each examination method
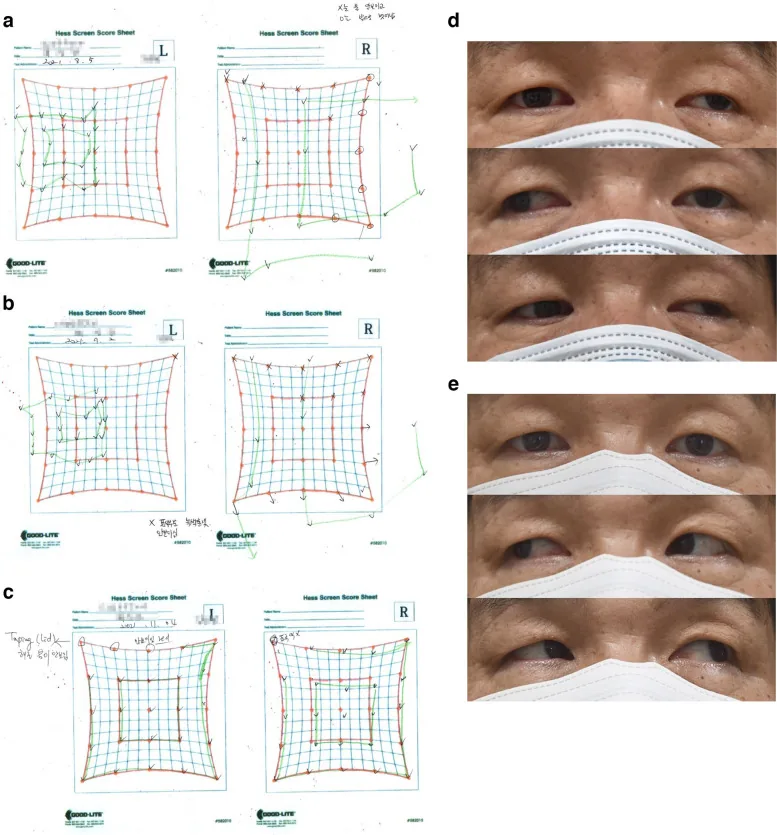
Kang K, Lee SY, Lee DC. Neuro-ophthalmologic symptoms after coronavirus disease 2019 vaccination: a retrospective study. BMC Ophthalmol. 2023;23(1):11. Figure 1. PMID: 36604664; PMCID: PMC9813886; DOI: 10.1186/s12886-022-02747-7. License: CC BY.
This shows the Hess screen test on day 4 (a), day 13 (b), and week 6 (c) after onset in a case of left oculomotor nerve palsy, together with external eye photographs of eye movements (d: −2 limitation in all directions except abduction, e: complete recovery in all directions). This corresponds to the visual inspection of eye movements and the serial Hess chart records described in section “3. Principles and procedures of each examination method.”
Version is conjugate eye movement in which both eyes move in the same direction, and eye movements in nine directions (straight ahead, right, left, up, down, upper right, lower right, upper left, lower left) are observed. Duction is eye movement assessed one eye at a time, and it is combined with the alternate cover test to confirm the direction of deviation.
Procedure for evaluating versions
Face the patient and perform the test at a distance of about 50 cm.
Use the examiner’s fingertip or a penlight to guide the eyes in nine directions.
Check how far the eyes can move in each direction and record whether there is any limitation.
Also check for overaction (such as dissociated nystagmus).
Ask the patient whether double vision occurs in each direction.
Procedure for evaluating ductions
Use alternate cover testing to judge the direction of deviation from eye movements after uncovering.
Check the range of movement of each eye one eye at a time.
Hess chart (Hess red-green test)
Principle: Separate the two eyes with red-green glasses, and detect eye position by superimposing a green target on the red grid.
Principle for interpretation: The smaller pattern indicates the paretic eye. The direction in which the pattern is smallest is the action direction of the paralyzed muscle
Indications: Quantitative recording of paralytic strabismus, follow-up of changes over time, preoperative and postoperative evaluation
Notes: If both eyes are paralyzed, it cannot be judged. In concomitant strabismus and skew deviation, the pattern size is the same in both eyes
Fixation field test
Monocular fixation field: Measures the range over which fixation can be maintained with one eye at a time. Normally, it is an almost 50° circle. Used to record duction
Binocular fixation field (single binocular field): Measures the range over which single vision is possible with both eyes. Normally, it is an almost 50° circle. Useful for understanding the direction and range of diplopia
Limitations: Rotational diplopia is not reflected. Diagnostic value is low; it is mainly useful as a record
Prepare the Hess chart (red grid screen or tablet) in a dark room
Have the patient wear red-green glasses (with the red lens on the fixation eye side)
The examiner points to each dot on the red screen (nine directions) in sequence
The patient aligns the green target
Record the deviation (in 9 directions)
Swap the red-green glasses between the right and left eyes and record again (record the opposite eye as the fixation eye)
Judge by comparing the patterns from both eyes
According to Hering’s law (muscles that work together receive equal innervation), the corresponding muscle in the opposite eye shows overaction (innervation sequelae). This is why the opposite-eye pattern enlarges on the Hess chart2).
Have the subject fixate straight ahead and slowly move the target toward the periphery
Record the angle limit at which single vision is maintained
Perform in 8 to 12 directions
Note that cyclotorsional diplopia is not reflected in the binocular fixation field
QWhat can the Hess chart show?
A
The Hess chart is used to identify the paretic eye, estimate the direction of the paretic muscle, and quantitatively record the degree of impairment. Patterns are recorded for both eyes; the smaller pattern indicates the paretic eye, and the direction with the greatest reduction indicates the action direction of the paretic muscle. Also, by Hering’s law, the corresponding muscle in the non-paretic eye becomes overactive, so the non-paretic eye’s pattern enlarges. However, if both eyes are affected, or in concomitant strabismus or skew deviation, interpretation requires caution.
Direct observation of eye movements provides more information, and the Hess chart and fixation field test are most valuable for follow-up and for recording changes before and after surgery.
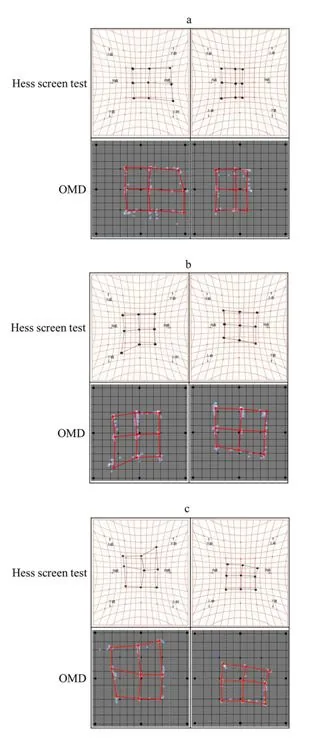
Iwata Y, Handa T, Ishikawa H. Objective measurement of nine gaze-directions using an eye-tracking device. J Eye Mov Res. 2020;13(6). Figure 5. PMID: 33828814; PMCID: PMC8015013; DOI: 10.16910/jemr.13.6.4. License: CC BY.
(a) Hess screen test pattern in right abducens nerve palsy, (b) right trochlear nerve palsy, and (c) superior oblique muscle dysfunction associated with thyroid eye disease. In each disease, the direction of narrowing in the affected-eye pattern differs and reflects the action direction of the paralyzed muscle. This corresponds to the Hess chart patterns for abducens nerve palsy, trochlear nerve palsy, and thyroid eye disease discussed in section 5.
The following shows the eye movement findings and Hess chart patterns in major diseases that cause eye movement disorders.
Skew deviation is one type of supranuclear eye movement disorder, in which one eye turns upward and the other turns downward (a vertical divergent eye position). It is seen with widespread brain damage, including the cerebellum and brainstem, and causes a comitant supranuclear vertical strabismus.
On the Hess chart, the pattern size is the same in both eyes, and only the deviation is recorded, which is different from paralytic strabismus. If skew deviation is suspected, neuroimaging (such as MRI) is essential3).
In comitant strabismus, the pattern size on the Hess chart is the same in both eyes, and only the horizontal or vertical deviation is recorded. In paralytic strabismus, by contrast, the pattern in the affected eye is clearly reduced. This difference is the most important criterion for judging the Hess chart.
6. Anatomy and innervation of eye movements (pathophysiology)
Lateral rectus (abduction muscle): Innervated by the abducens nerve (cranial nerve VI)
Superior oblique: Innervated by the trochlear nerve (cranial nerve IV)
Medial rectus, superior rectus, inferior rectus, and inferior oblique: Innervated by the oculomotor nerve (cranial nerve III)
Remembering that only the lateral rectus is supplied by the abducens nerve, and only the superior oblique by the trochlear nerve, is useful for diagnosing cranial nerve palsy.
The following two basic laws apply to eye movements2).
Hering’s law: yoked muscles (the muscles in both eyes that handle movement in the same direction) receive equal innervation. When innervation to the paralyzed eye increases, the same amount of innervation also goes to the same-direction muscle in the non-paralyzed eye, causing the non-paralyzed eye to overact
Sherrington’s law: when the eye moves in one direction, the agonist contracts while the antagonist relaxes (reciprocal innervation)
Eye movement disorders are classified into three levels according to the level of damage.
Infranuclear (lower motor neuron) lesion: a lesion between the cranial nerve nucleus and the muscle. Paralysis of an individual muscle may occur, while conjugate movements may be preserved
Nuclear lesion: a lesion of the cranial nerve nucleus. Because of the structural arrangement within the nucleus, it is often accompanied by other neurological symptoms
Supranuclear (upper motor neuron) lesion: impairment of conjugate movement. Internuclear ophthalmoplegia (MLF syndrome) results from a lesion of the medial longitudinal fasciculus (MLF) and causes ipsilateral adduction limitation and dissociated nystagmus on contralateral abduction3)
Because MLF syndrome is a disorder of conjugate movement rather than paralysis of an individual extraocular muscle, the Hess chart shows a complex pattern. A detailed neuro-ophthalmic evaluation is needed.
Horizontal eye movements are controlled by the pontine paramedian reticular formation (PPRF) and the abducens nucleus, and vertical eye movements are controlled by the interstitial nucleus of the midbrain (riMLF). If these supranuclear control circuits are damaged, conjugate eye movements in a specific direction are impaired3).
The VOR, OKN, saccade, and smooth pursuit systems work together to produce accurate eye movements. Evaluation of these systems is part of advanced neuro-ophthalmic testing.
In addition to conventional optical screen Hess charts, development and use of tablet- and PC monitor-based digital Hess charts are advancing1). Digitalization makes it easier to automate test records and integrate them into electronic medical records, and it is expected to improve the accuracy of tracking changes over time.
Video eye movement measurement (Video-oculography)
Video-oculography (VOG), which combines an infrared camera with eye-tracking technology, makes it possible to measure eye movements quantitatively in three dimensions. It can measure horizontal, vertical, and torsional components at the same time, helping to overcome the limits of gaze field examination, which cannot reflect torsional diplopia2).
Automation of strabismus quantification with AI analysis
Eye movement analysis using machine learning and deep learning is being studied, and algorithms that automatically identify the paralyzed muscle from Hess chart patterns are being developed. In the future, these methods are expected to be used in telemedicine and in eye movement assessment at general clinics.
Research is progressing on remote eye movement assessment using cameras on smart devices. Its use in triage for acute ocular motor palsy and in neuro-ophthalmology consultations is being considered, but ensuring quantitative accuracy remains a challenge.