Orbital floor fracture, also called blowout fracture, is defined as a fracture of the orbital floor with preservation of the inferior orbital rim.
When blunt force is applied to the eye, the bones forming the orbit may fracture. The inferior and medial walls are very thin and are common sites for this condition, often with large bone displacement toward the paranasal sinuses. This morphology is also called orbital blowout fracture.
Isolated orbital wall fractures account for about 10% of all facial fractures, with the majority occurring in the orbital floor. The orbit is involved in 30–40% of all facial fractures. Isolated orbital floor fractures account for 22–47% of all orbital fractures. 2)
In terms of sex and age distribution of injured patients (analysis of 268 cases), 72% were male and 28% female, with an average age of 36 years. 2)
As a structural characteristic of the orbital floor, the bone thickness at the site of the infraorbital neurovascular bundle is only 0.23 mm, and the posteromedial bone thickness averages 0.37 mm, which is extremely thin. The lateral side has an average thickness of 1.25 mm, more than five times thicker. The medial orbital wall and infraorbital groove are also particularly thin and are common sites of fracture.
Fractures are classified into open and closed types based on imaging findings.
Open type: Bone fragments and soft tissue are significantly displaced into the paranasal sinuses.
Closed type (trapdoor type): Imaging changes are subtle, and a characteristic finding is soft tissue entrapped in a slightly displaced fracture (missing rectus sign). The closed type is more common in young people and children.
In children, the incidence is high due to thin bone walls. The main causes are falls, blows from one’s own or another’s knee, traffic accidents, and punches with a fist. The most common sites are the maxilla and ethmoid bone, with the orbital floor being the most frequent.
QIs an orbital floor fracture the same as a blowout fracture?
A
They are essentially synonymous. “Blowout fracture” refers to the phenomenon where a blow to the eye increases intraorbital pressure, causing the thinnest part of the orbital floor to blow out. Orbital floor fracture is a term indicating the typical fracture site and is used as a translation of blowout fracture.
Diplopia: Occurs due to impaired eye movement. It worsens with vertical eye movements.
Enophthalmos: Progresses over several days to weeks after injury as swelling subsides.
Eye pain: Characteristically occurs during vertical eye movements.
Hypesthesia and paresthesia: In inferior wall fractures, the infraorbital groove may be involved. Paralysis of the second branch of the trigeminal nerve causes hypesthesia and paresthesia from the cheek to the upper lip on the affected side.
Characteristics of findings by fracture type are shown below.
Open Fracture
Displacement of bone fragments: Bone fragments and soft tissue are significantly displaced into the paranasal sinuses.
Enophthalmos: The eyeball moves posteriorly due to expansion of the orbital volume. Enophthalmos becomes more noticeable as swelling subsides after injury.
Prognosis: If there is no incarceration, the prognosis for eye movement is relatively good.
Closed Fracture
Subtle imaging changes: Slight displacement at the fracture site and the missing rectus sign are characteristic findings.
Associated systemic symptoms: Vagal reflex due to tissue incarceration causes severe eye pain, nausea, vomiting, syncope, and bradycardia. It may be misdiagnosed as increased intracranial pressure.
High urgency: If accompanied by extraocular muscle entrapment, there is a risk of muscle necrosis, and emergency surgery is indicated.
In closed fractures, a crack occurs in the bone due to external force, and when the displaced bone attempts to return to its original shape, the extraocular muscles or perimuscular soft tissue become entrapped in the crack. It is characterized by a tendency to be accompanied by systemic symptoms such as severe eye pain, nausea, vomiting, syncope, and bradycardia due to vagal reflex. If there is tissue incarceration at the fracture site, vertical eye movements may cause nausea and bradycardia (oculocardiac reflex).
QWhy does diplopia occur in orbital floor fractures?
A
The main cause is restriction of movement due to entrapment of extraocular muscles and orbital tissues in the fracture site. Even if only the orbital septa within the orbital fat are caught near the extraocular muscles, eye movement restriction can occur. The cause of diplopia is not the fracture alone, but a combination of factors including trauma, soft tissue injury, fibrosis, and nerve contusion. 1)
QWhy do vomiting and syncope occur in closed fractures?
A
In closed (trapdoor) fractures, the extraocular muscle is strangulated and entrapped in the fracture site. Attempting to move the eye strongly pulls the entrapped muscle, triggering a vagal reflex. This results in severe eye pain, nausea, vomiting, syncope, and bradycardia. It may be misdiagnosed as intracranial pathology or gastrointestinal disease, so careful differentiation is necessary.
Blunt trauma to the eye and periorbital area is the cause. Analysis of 268 cases: assault 35.1% (most common), falls 21.6%, sports 19.0%, traffic accidents 13.8%, workplace accidents 1.1%. 2)
There are two theories regarding the mechanism of fracture.
Hydraulic theory: A fist or ball directly strikes the eye, causing a rapid increase in intraorbital pressure and blowout at the weakest point (just above the infraorbital neurovascular bundle). Fractures due to increased intraorbital pressure correspond to this.
Buckling theory: A blow to the cheek transmits a pressure wave posteriorly, causing anteroposterior bone compression and buckling at the weakest point, pushing the bone fragment downward. This corresponds to a contrecoup fracture (fracture at a site distant from the impact point).
Both theories are considered valid based on cadaver studies.
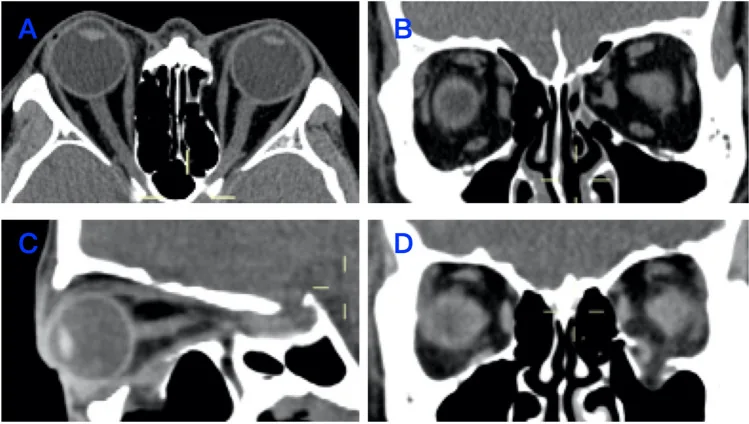
Yang J, et al. Insights into orbital morphological features and fracture patterns in medial and inferior wall fracture: a retrospective cohort study. Sci Rep. 2023. Figure 1. PMCID: PMC10681974. License: CC BY 4.0.
Representative CT images of orbital wall fractures. (A) Axial view of medial wall fracture, (B) Coronal view of medial wall fracture, (C) Sagittal view of orbital floor fracture, (D) Coronal view of orbital floor fracture. Corresponds to the orbital CT diagnosis discussed in section “4. Diagnosis and Examination Methods.”
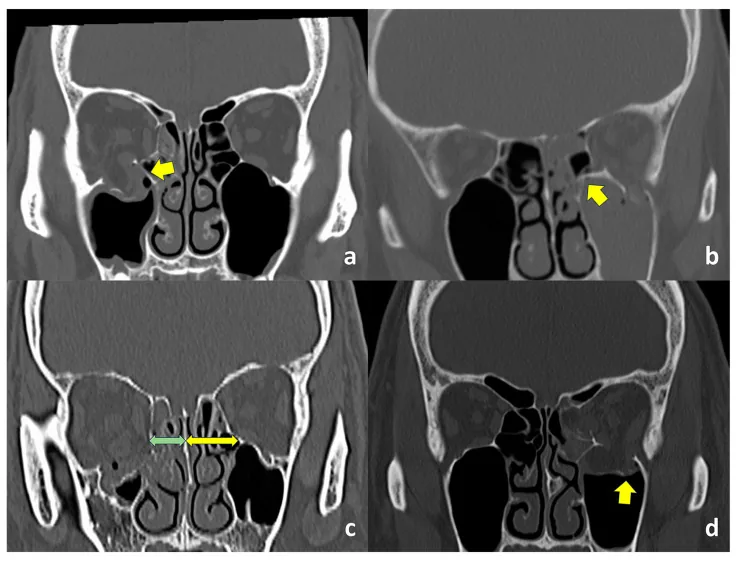
Someda SK, et al. Clinical Significance of the Inferomedial Orbital Strut in Orbital Blowout Fractures: Incidence of Symptomatic Diplopia in a Fractured vs. Intact Strut. J Clin Med. 2024. Figure 1. PMCID: PMC11242313. License: CC BY.
CT findings: (a) intact inferomedial orbital strut, (b) fractured strut, (c) distance between the junction of the orbital floor and medial wall and the nasal septum is shorter on the affected side (green arrow) than on the unaffected side (yellow arrow), (d) orbital floor fracture lateral to the infraorbital groove. Shows the clinical association between inferomedial orbital strut fracture and diplopia.
A complete ophthalmic examination is essential. The first step is to rule out vision-threatening complications such as globe rupture and retinal detachment.
Orbital CT is mandatory for definitive diagnosis. When performing CT, instruct the radiology department to obtain both bone and soft tissue windows.
CT bone window: Useful for observing subtle fractures. Allows accurate assessment of fracture morphology.
CT soft tissue window: Useful for detailed observation of the positional relationship between bone and soft tissue, as well as displacement, herniation, incarceration, and strangulation.
Coronal and sagittal views: Essential for detailed assessment of the orbital floor fracture. Axial views alone are insufficient; reconstructed coronal and sagittal views are useful.
MRI: Used as a complement when detailed observation of soft tissue is needed.
An increase in orbital volume of 13% or more carries a high risk of enophthalmos. Note that radiological herniation of the inferior rectus muscle does not necessarily predict clinical motility disturbance.
Hess chart and binocular single vision field test: Objectively evaluate eye movement and diplopia.
Forced duction test: Surgical indication can be adequately determined based on imaging and clinical findings; this test is not recommended to be performed actively because it is painful when performed under local anesthesia.
Differential diagnoses include orbital congestion, extraocular muscle palsy, nerve palsy, diplopia due to loss of fusion, and medial orbital wall fracture. Note that incarceration is a purely clinical diagnosis, not a radiological one.
Closed fractures with extraocular muscle entrapment (trapdoor fractures) carry a risk of muscle necrosis and require emergency reduction within 24 hours of injury. On the other hand, for mild open fractures where reversible changes are predominant, observation may be chosen.
In large open fractures, edema may subside about 2 weeks after injury, and enophthalmos may become prominent. Prior explanation to the patient is important.
Performed under general anesthesia. The orbital rim periosteum is reached percutaneously or transconjunctivally, and after periosteal incision, the surgical field is expanded posteriorly into the orbit. Specifically, the infraorbital rim is reached via a subciliary skin incision or an inferior fornix conjunctival incision (transconjunctival approach).
All soft tissues that have herniated into the paranasal sinuses due to the fracture are reduced back into the orbit. Displaced bone fragments are returned to their original position and reconstructed using bone reconstruction materials or artificial bone. Damaged periosteum is reconstructed with silicone plates or absorbable plates.
In children, a transconjunctival fornix incision approach is also used. Fracture repair is performed with bone fragments if possible; in comminuted fractures, reconstruction materials are used to fill the defect. A transmaxillary sinus (paranasal sinus) approach is also an option.
Steroids: Short-term administration. Prednisone 0.75–1.0 mg/kg/day for 5–7 days. Alternatively, intraoperative Decadron 20 mg IV, followed by prednisone 0.75–1.0 mg/kg/day for 3–5 days.
Antibiotics: May be prescribed in the acute phase. Perioperative antibiotic prophylaxis is common, with amoxicillin-clavulanate being the most frequently used.2)
A systematic review of 444 cases reported that surgery improved enophthalmos in 85.2%, diplopia in 74.8%, restricted eye movement in 61.6%, and sensory disturbance in 61.1%.2)
If reduction surgery is performed early with an appropriate technique, the prognosis is generally good. Prognosis varies depending on the extent of tissue damage, timing of surgery, and surgical technique.
QIs surgery always necessary for orbital floor fractures?
A
Surgery is not always necessary. Mild diplopia and motility disturbances often improve spontaneously, and observation may be chosen. Closed fractures with extraocular muscle entrapment, persistent diplopia, and enophthalmos are the main indications for surgery.
Two mechanisms have been proposed for the occurrence of orbital floor fractures, both validated in cadaver studies.
Hydraulic Theory
Increased intraorbital pressure due to impact: A fist or ball directly strikes the eye, displacing the globe posteriorly.
Rupture of the weakest area: The sudden rise in intraorbital pressure causes the thinnest areas (floor and medial wall) to blow out.
Soft tissue herniation: Orbital contents (fat and muscle) herniate into the paranasal sinuses through the fracture.
Buckling Theory
Propagation of pressure waves: A pressure wave generated by blunt trauma to the cheek propagates posteriorly through the bone.
Bone compression and buckling: Anteroposterior bone compression causes the weakest part of the orbital floor to buckle, pushing bone fragments downward (contrecoup fracture).
Direct bone deformation: Unlike the hydraulic theory, direct impact to the globe is not necessarily required.
The mechanisms of diplopia and ocular motility disturbance are as follows:
Restriction of extraocular muscle movement: Entrapment of the extraocular muscle at the fracture site is the main cause. Damage or strangulation of the extraocular muscle itself also causes severe contractile dysfunction.
Entrapment of orbital septa: Orbital septa run vertically and horizontally within the orbital fat, and even if a septum near an extraocular muscle is caught in the fracture site, it can cause restriction of eye movement.
Multifactorial causes: The cause of diplopia is not solely the fracture but a combination of factors including trauma, soft tissue injury, fibrosis, and nerve contusion. 1)
The mechanism of enophthalmos is as follows. Herniation of orbital tissue into the paranasal sinuses through the fracture expands the orbital volume, causing the eyeball to move posteriorly, resulting in enophthalmos.
7. Latest Research and Future Perspectives (Investigational Stage)
The use of custom-made implants tailored to individual fracture patterns based on CT images is advancing.
A reduction in surgical time has been reported, with significant shortening in the preformed group (57.3±23.4 minutes) compared to the freehand molding group (99.8±28.9 minutes). 2)
Endoscopic transnasal and transmaxillary approaches are associated with less soft tissue damage and less infraorbital nerve hypoesthesia compared to conventional transcutaneous approaches. 2)
In a narrative review of 66 studies and 3870 cases by Sivam & Enninghorst (2022), neobone formation was confirmed after complete absorption of Poly-L/D-lactic acid, and a study of 94 cases reported significant improvement in eye movement, diplopia, and enophthalmos. 3)
A systematic review by de Santana et al. (2024) concluded that definitive evidence of a direct association between orbital floor fractures and ocular motility disorders is currently insufficient. 1) Further elucidation of the pathophysiology through multicenter collaborative studies is needed.
de Santana IHG, Viana MRM, Palhano-Dias JC, Ferreira-Júnior O, Sant’Ana E, Shinohara ÉH, et al. Orbital floor fracture (blow out) and its repercussions on eye movement: a systematic review. European journal of medical research. 2024;29(1):427. doi:10.1186/s40001-024-02023-y. PMID:39164786; PMCID:PMC11334373.
Miran B, Toneatti DJ, Schaller B, Kalaitsidou I. Management Strategies for Isolated Orbital Floor Fractures: A Systematic Review of Clinical Outcomes and Surgical Approaches. Diagnostics (Basel, Switzerland). 2025;15(23). doi:10.3390/diagnostics15233024. PMID:41374405; PMCID:PMC12690994.
Sivam A, Enninghorst N. The Dilemma of Reconstructive Material Choice for Orbital Floor Fracture: A Narrative Review. Medicines (Basel, Switzerland). 2022;9(1). doi:10.3390/medicines9010006. PMID:35049939; PMCID:PMC8778999.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.