An orbital medial wall fracture is a fracture of the lamina papyracea, which forms the medial wall of the orbit. The inferior and medial walls of the orbit have very thin bone and are common sites for this condition. The lamina papyracea is as thin as 0.2 mm at its thinnest point and is vulnerable to blunt force.
Isolated fractures are relatively rare; most occur together with an orbital floor fracture or as part of a combined fracture. They may also be associated with fractures of the frontal bone, nasoethmoidal region, and maxilla. Orbital fractures that do not involve the orbital rim are called “blow-out fractures.”
The cause is almost always blunt trauma to the periorbital area. Common mechanisms include traffic accidents, sports activities, violence, falls, and trip-and-fall accidents. It is more common in men, and contact sports are a typical risk factor. Fracture patterns vary by age depending on facial development and pneumatization of the paranasal sinuses.
Orbital medial wall fracture and orbital floor fracture (09-24) are both types of blow-out fractures, but they differ in the affected sinus, the entrapped extraocular muscle, and the resulting symptoms.
QHow is a medial orbital wall fracture different from an orbital floor fracture?
A
An orbital floor fracture is a fracture of the orbital floor (maxillary bone), while a medial orbital wall fracture is a fracture of the lamina papyracea of the ethmoid bone. The two often occur together. Orbital floor fractures frequently cause sensory disturbances in the infraorbital nerve area, whereas medial orbital wall fractures primarily cause horizontal eye movement disorders due to entrapment of the medial rectus muscle.
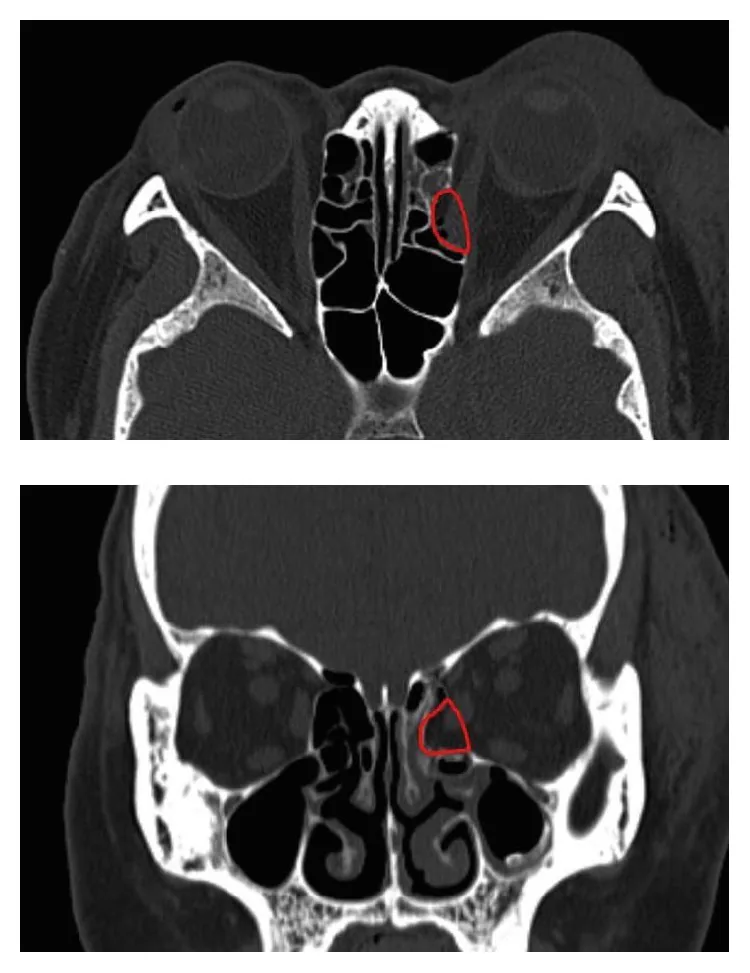
Shin J, et al. Reconstruction of Medial Wall Blowout Fracture Defect with a Combination of Resorbable Meshed Plate and Cancellous Bone Allograft. Biomed Res Int. 2019. Figure 1. PMCID: PMC6815640. License: CC BY.
Based on CT images, the 3D shape of the bone defect is estimated, and the red line indicates the defect area to be replaced by cancellous bone allograft using the inlay technique. This corresponds to the medial orbital wall fracture discussed in the section “2. Main symptoms and clinical findings.”
Isolated medial wall fractures may be asymptomatic.
Diplopia: Occurs during horizontal gaze. Entrapment of the medial rectus muscle causes abduction limitation, and horizontal diplopia due to fixed adduction is characteristic. Even without entrapment, it can occur due to soft tissue swelling or muscle contusion.
Epistaxis (nosebleed): Blood accumulated in the paranasal sinuses due to the fracture flows into the nasal cavity.
Pain with eye movement: Occurs in cases with entrapment.
Subcutaneous emphysema: Periorbital swelling worsens after blowing the nose. This is an important symptom suggesting communication between the orbit and the nasal cavity. Forceful nose blowing after injury can cause orbital emphysema, worsening eyelid swelling and eye movement disorders.
Oculocardiac reflex: Can occur in children and young adults with entrapment. Symptoms include nausea, vomiting, bradycardia, dizziness, and fainting. It is caused by a vagal reflex. In closed fractures, it may be misdiagnosed as increased intracranial pressure, leading to delayed diagnosis.
QWhy did the area around my eye swell after blowing my nose?
A
When the medial orbital wall is fractured, creating a communication between the orbit and the paranasal sinuses, blowing the nose forces air into the orbit, causing orbital emphysema. This rapidly worsens periorbital swelling. Patients are advised not to blow their nose for two weeks after the fracture.
Clinical findings (findings confirmed by the physician during examination)
Ocular motility disorder: Horizontal eye movement is restricted in both adduction and abduction. Abduction limitation due to entrapment of the medial rectus muscle is prominent, and the eye becomes fixed in adduction depending on the degree of incarceration. It worsens with orbital hemorrhage or emphysema.
Enophthalmos: Measured with a Hertel exophthalmometer. It may be masked by soft tissue swelling in the early stage. In large open fractures, it becomes noticeable about 2 weeks after injury as edema subsides. Repeated measurements during follow-up are important.
Orbital emphysema: In medial wall fractures, air inflow from the ethmoid sinus is particularly prominent. Even a small amount of emphysema can cause severe limitation of eye movement in all directions. It is absorbed spontaneously within a few days.
Palpation findings: Check for crepitus indicating emphysema and step-off deformity.
Retrobulbar hemorrhage: Rare but can occur in severe cases. It causes painful proptosis, elevated intraocular pressure, and vision loss due to optic nerve compression, requiring emergency intervention as orbital compartment syndrome.
Systemic evaluation of the oculocardiac reflex: Especially in children and young adults with extraocular muscle entrapment, assess for bradycardia, nausea, vomiting, syncope, and heart block.
QWhy do children with medial orbital wall fracture vomit?
A
When an extraocular muscle is entrapped in the fracture site, the oculocardiac reflex (vagal reflex) occurs, causing nausea, vomiting, and bradycardia. These symptoms are easily mistaken for increased intracranial pressure, leading to delayed diagnosis as patients are transferred to neurosurgery or pediatrics. In children presenting with vomiting after trauma, orbital fracture should be actively suspected6).
The pathogenesis of medial orbital wall fracture involves two theories: the hydraulic hypothesis and the buckling theory. In many cases, it occurs through a combination of both mechanisms.
Hydraulic Hypothesis
Mechanism: External impact around the orbit → increased intraorbital pressure → pressure transmitted to the orbital floor and medial wall → fracture.
Evidence: The lateral wall and orbital roof are thick enough to withstand, but the thin medial wall and floor fail first.
Buckling Theory
Mechanism: Direct force to the orbital rim → transmitted to the more vulnerable orbital floor and medial wall → fracture.
Rationale: Force on the orbital rim propagates through the orbital wall and concentrates at weak areas.
Medial orbital wall fractures are particularly likely to occur with medial forces such as a blow to the nasal bridge. Fracture types are classified as comminuted, hinge, blow-in, and trapdoor. Comminuted fractures are most common, with bone fragments and orbital contents herniating into the ethmoid sinus. Closed fractures are more common in young patients, where the bone returns to its original shape and can entrap extraocular muscles or soft tissues in the crack.
Orbital CT (computed tomography) is the primary tool for diagnosing fractures. It is used to evaluate the location and size of the fracture, extraocular muscle entrapment, and retrobulbar hemorrhage. It is also essential for planning surgical repair. Imaging including coronal and sagittal views is mandatory to check for soft tissue herniation into the ethmoid sinus and entrapment of the medial rectus muscle.
The characteristics of each imaging method are shown below.
CT should include both soft tissue windows (to assess position, displacement, herniation, entrapment, and strangulation of bone and soft tissue) and bone windows (to detect subtle fractures). Herniation of orbital fat into the ethmoid and maxillary sinuses is confirmed on soft tissue CT. Opacification of the ethmoid sinus may also be seen on plain X-ray, but sensitivity is low and the information obtained does not justify radiation exposure. MRI is not the first choice after trauma due to concern for unknown metallic intraocular foreign bodies.
Axial CT is standard, but if coronal views are useful, they can be obtained by three-dimensional reconstruction. Brain windows may not display orbital fat; switching to soft tissue windows (adjusting window width) makes it easier to assess orbital fat and orbital emphysema.
Imaging classification includes open type (bone fragments and soft tissue are significantly displaced into the sinus) and closed type (imaging changes are subtle, with soft tissue entrapped in a minimally displaced fracture, missing rectus sign).
A history of periorbital trauma combined with horizontal gaze limitation, emphysema, and enophthalmos suggests a medial wall fracture. Confirmation is by radiological examination.
For evaluation of diplopia, use the cover test, binocular single vision field test, and Hess red-green test (most precise). The Hess chart shows an internal rectus palsy pattern (abduction limitation) and assesses the degree of entrapment.
Periorbital ecchymosis without fracture (gaze limitation not restricted to horizontal gaze)
Post-traumatic muscle palsy, hemorrhage, or contusion (mimicking entrapment)
Complications of optic canal fracture, skull base fracture, facial bone fracture, and ocular injury
QWhy is CT preferred over MRI?
A
After trauma, there may be intraocular metallic foreign bodies, and MRI is not the first choice from a safety perspective. CT is excellent for bone visualization and is most suitable for evaluating fractures, entrapment, and retrobulbar hemorrhage. MRI is used adjunctively when additional evaluation such as paranasal sinus mucocele is needed.
Conservative treatment is indicated in the following cases:
Good extraocular muscle movement with minimal diplopia
Insignificant enophthalmos (<2 mm, cosmetically acceptable)
Diplopia without entrapment (may resolve spontaneously)
Mild ocular movement disorder/diplopia with reversible imaging changes
Basic guidance for conservative treatment includes instructing the patient not to blow their nose within 2 weeks after injury. This is to prevent orbital emphysema and invasion of non-sterile sinus contents into the orbital cavity. The role of antibiotics is controversial. Steroids (prednisolone 1 mg/kg for 10 days) have been reported to reduce edema and facilitate identification of patients with entrapment. Orbital emphysema usually resolves spontaneously within 1-2 weeks.
Symptomatic diplopia with positive forced duction test
Ideally within 2 weeks
Early surgery
CT evidence of extraocular muscle incarceration
Promptly
Early surgery
Open fracture with irreversible ocular motility disorder
Reposition before scarring
Elective surgery
Enophthalmos due to large fracture
Possible even after 2 weeks
Surgery may be postponed if there is concurrent globe rupture, intraocular injury, or medical comorbidities. Even in chronic cases, surgery may be indicated, as determined by imaging.
Delaying surgery worsens prognosis. Repair within 14 days results in an enophthalmos residual rate of about 20%, whereas repair after 6 months or more results in about 72% residual. Studies on surgical timing report that the rate of diplopia resolution was 58% in patients who underwent surgery within 2 weeks, compared to 38.1% after 4 weeks. A systematic review and meta-analysis of 442 cases by Damgaard et al. also showed a significantly increased odds ratio of 3.3 for residual postoperative diplopia in the delayed surgery group after 14 days 2).
Indications: Combined medial wall and orbital floor fractures.
Incision: Subciliary incision or transconjunctival incision (for inferior medial wall), transcaruncular approach or transcanthal incision (Lynch incision) or Kroum incision (for isolated medial wall fracture). The transcaruncular approach leaves no skin scar, allows wide exposure from the medial wall to the orbital floor, and has a low complication rate 3) 4).
Complications: Eyelid malposition, infraorbital nerve hypoesthesia (improves in 2–8 weeks). Subciliary incision carries a risk of cicatricial ectropion. Lynch incision requires attention to scarring at the medial canthus.
Advantages: Slight benefits in operative time, hospital stay, and cost.
Endoscopic approach
Procedure: Uncinate process resection → ethmoidectomy → identification of fracture site → reduction of herniated tissue → implant insertion (e.g., Silastic, Merocel, Medpor).
Confirmation: Forced duction test and pulse test are used to confirm eye movement and implant placement.
Complications: Maxillary sinusitis (due to sinus drainage obstruction), migration of bone fragments into the orbit, and need for postoperative nasal packing. If the implant is too large, complications including extrusion increase.
Advantages: Can be used for early repair, less traction on the eyeball. Suitable for medial wall fractures and trapdoor fractures. Not usable for large defects 5).
The orbital rim periosteum is reached percutaneously or transconjunctivally. After periosteal incision, the surgical field is developed posteriorly. Herniated orbital fat and medial rectus muscle are reduced, bone fragments are restored to their original position, and the bone wall is reconstructed using artificial bone or absorbable plates. Absorbable implants made primarily of bioabsorbable polymer (poly-L-lactic acid PLLA) or silicone sheets are widely used to reconstruct the orbital wall.
QDoes surgery need to be performed urgently?
A
In closed fractures with proven extraocular muscle entrapment, emergency surgery within 24 hours of injury is necessary due to the risk of muscle necrosis. On the other hand, in cases without incarceration, surgery can be delayed for up to 2 weeks. Since surgical delay worsens prognosis, the decision for surgery should be made promptly.
The medial orbital wall is the thinnest of the orbital walls, mainly formed by the lamina papyracea. By definition, a blow-out fracture is a pure internal fracture that does not involve the orbital rim. When intraorbital pressure increases, the thinnest lamina papyracea breaks first, and the medial rectus muscle and orbital fat become incarcerated in the ethmoid sinus.
The pathophysiology by fracture type is as follows.
Open fracture: Bone fragments are significantly displaced into the paranasal sinuses. Orbital fat herniates into the ethmoid and maxillary sinuses. Moderate restriction of eye movement and enophthalmos tend to persist, and surgical indication should be actively considered.
Closed fracture (trapdoor type): More common in young people. When the bone returns to its original shape, the extraocular muscles and surrounding soft tissues become entrapped in the crack. Severe restriction of eye movement occurs, and emergency surgery is indicated.
Comminuted fracture: Bone fragments and orbital contents (extraocular muscles, fat, soft tissue) herniate into the ethmoid sinus.
Trapdoor fracture: The bone fragment opens and closes, trapping tissue.
Blow-in fracture: A bone fragment protrudes into the orbit.
The mechanism of enophthalmos involves herniation of orbital contents into the paranasal sinuses, which increases orbital volume and causes posterior displacement of the globe. Enophthalmos occurs when orbital volume increases by 13% or more.
Orbital fat contains thin septa (orbital septa). When the septa near the extraocular muscles are trapped, restriction of eye movement can occur even without entrapment of the muscle itself. Severe strangulation of the medial rectus muscle can lead to muscle necrosis and permanent abduction limitation (horizontal diplopia). Early reduction surgery can improve diplopia and enophthalmos, but if medial rectus necrosis occurs, permanent diplopia results.
Yu DY, Chen CH, Tsay PK, Leow AM, Pan CH, Chen CT. Surgical Timing and Fracture Type on the Outcome of Diplopia After Orbital Fracture Repair. Ann Plast Surg. 2016;76 Suppl 1:S91-5. PMID: 26808744.
Damgaard OE, Larsen CG, Felding UA, Toft PB, von Buchwald C. Surgical Timing of the Orbital “Blowout” Fracture: A Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg. 2016;155(3):387-90. PMID: 27165680.
Nguyen DC, Shahzad F, Snyder-Warwick A, Patel KB, Woo AS. Transcaruncular Approach for Treatment of Medial Wall and Large Orbital Blowout Fractures. Craniomaxillofac Trauma Reconstr. 2016;9(1):46-52. PMID: 26889348; PMCID: PMC4755730.
Lee K, Snape L. Efficacy of Transcaruncular Approach to Reconstruct Isolated Medial Orbital Fracture. J Maxillofac Oral Surg. 2010;9(4):355-8. PMID: 22190773; PMCID: PMC3244106.
Bonsembiante A, Valente L, Ciorba A, Galiè M, Pelucchi S. Transnasal Endoscopic Approach for the Treatment of Medial Orbital Wall Fractures. Ann Maxillofac Surg. 2019;9(2):248-251. PMID: 31909026; PMCID: PMC6933993.
Basnet A, Chug A, Simre S, Vyas A, Shrestha S. Comprehensive Management of Pediatric Orbital Fractures: A Case Series and Review of Literature. Cureus. 2024;16(4):e57842. PMID: 38725748; PMCID: PMC11081518.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.