ZMC fracture (Zygomaticomaxillary Complex Fracture) is a facial injury in which the zygomatic bone fractures simultaneously at four articulations with adjacent bones. The four fracture sites are as follows:
Zygomatic arch: the arch-shaped bone connecting the zygomatic bone and temporal bone
Frontozygomatic suture: the junction between the zygomatic bone and frontal bone
Infraorbital rim (junction with the maxilla): the orbital rim below the eye
Orbital floor: the bottom of the orbit that supports the eyeball
Because these four sites are injured simultaneously, an orbital floor fracture is inevitably involved. When the orbital floor is fractured, orbital contents may herniate into the paranasal sinuses, causing enophthalmos and diplopia due to extraocular muscle entrapment. Therefore, ZMC fracture is not only a maxillofacial surgical problem but also a trauma requiring ophthalmologic management.
ZMC fractures are caused by direct force to the cheek. Common mechanisms include traffic accidents, violence, sports injuries, and falls. They are relatively frequent among facial fractures and are more common in adult men.
Severe facial trauma such as from traffic accidents may be accompanied by fractures of the nasal bone, zygomatic arch, skull base, and other craniofacial bones, making collaboration with otolaryngology and neurosurgery important. The following specialties are involved in ZMC fractures:
Plastic Surgery / Otolaryngology: Main department responsible for reduction of the zygomatic bone (plate fixation, zygomatic arch elevation).
Ophthalmology: Responsible for reduction of orbital floor fractures, eye protection, and evaluation and follow-up of eye movement.
Neurosurgery: Involved when there are concomitant skull base fractures or intracranial injuries.
QWhat is the difference between ZMC fracture and orbital floor fracture?
A
An orbital floor fracture refers to a fracture of only the inferior wall of the orbit. A ZMC fracture is a complex fracture involving simultaneous fractures at four sites where the zygomatic bone articulates (zygomatic arch, frontozygomatic suture, infraorbital rim, and orbital floor). The orbital floor fracture is one component of a ZMC fracture. ZMC fractures cause not only ophthalmic problems but also plastic surgical issues such as trismus and facial deformity, making multidisciplinary collaboration essential.
Symptoms of ZMC fractures are broadly divided into ophthalmic symptoms and facial surgical symptoms.
Ophthalmic Findings
Diplopia: Caused by entrapment of the inferior rectus muscle or orbital fat in the fracture site of the orbital floor. It is exacerbated by vertical eye movements.
Enophthalmos: Orbital contents herniate into the paranasal sinuses due to orbital floor fracture, expanding the orbital volume and causing posterior displacement of the globe. It becomes more prominent as post-injury edema subsides.
Eyelid swelling and ecchymosis: Occur immediately after injury. As edema resolves, enophthalmos and diplopia become more apparent.
Ocular motility restriction: Caused by entrapment of extraocular muscles or orbital fat septa in the fracture site. Particularly, downward and upward gaze are limited.
Facial surgical findings
Pain on mouth opening and trismus: Depressed bone fragments from a zygomatic arch fracture compress the temporalis and masseter muscles, causing these symptoms.
Sensory abnormalities of the cheek: Injury to the infraorbital nerve (peripheral branch of the second division of the trigeminal nerve) causes hypoesthesia or paresthesia from the affected cheek to the upper lip.
Flattening of the cheek: The zygomatic bone is displaced inward and downward, resulting in loss of cheek prominence when viewed from the front. The appearance is as if the high cheekbone has disappeared.
Orbital emphysema: Blowing the nose can force air from the paranasal sinuses into the orbit, worsening eyelid swelling and eye movement impairment.
If the extraocular muscles or orbital tissues are entrapped (severe incarceration in the fracture site), vertical eye movements may trigger nausea, bradycardia, or syncope. This is particularly prominent in children and may be misdiagnosed as increased intracranial pressure, requiring caution.
ZMC fractures result from direct force to the cheek. The zygomatic bone is fixed at four sutures with the temporal, frontal, and maxillary bones. When strong force is applied, all four sutures are simultaneously disrupted, and the entire zygomatic bone collapses inward and downward.
The main mechanisms of injury are as follows:
Traffic accidents: Strong impact to the face from car, motorcycle, or bicycle accidents
Assault: Punching to the cheek is one of the most common mechanisms of injury
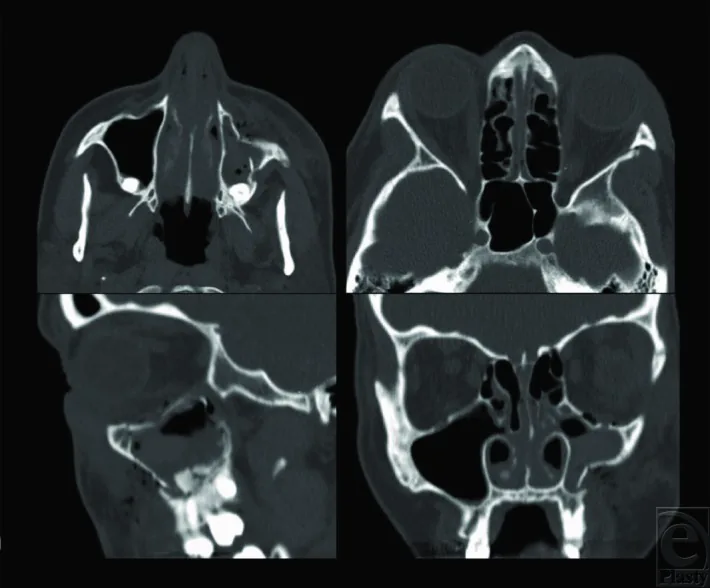
Gerbino G, et al. Zygomaticomaxillary Complex Fracture. ePlasty. 2014;14:ic27. Figure 1. PMCID: PMC4145677. License: CC BY.
Preoperative CT images of zygomaticomaxillary complex (ZMC) fracture (four-panel display). The upper left axial view shows depression of the zygoma and loss of projection; the upper right axial view shows separation at the sphenozygomatic suture; the lower left and lower right coronal views show fractures at the zygomaticomaxillary suture and orbital floor. This corresponds to the multi-planar diagnosis of ZMC fracture using orbital CT discussed in section “4. Diagnosis and examination methods.”
Diagnosis of ZMC fracture is made by combining imaging studies and ophthalmic functional evaluation. It is important to first rule out complications that threaten vision, such as globe rupture or retinal detachment.
Hess chart: Objectively evaluate eye movements and record the location and degree of extraocular muscle palsy
Binocular single vision test: Quantitatively evaluate the range of diplopia
Forced duction test: Confirm the presence of extraocular muscle entrapment. This test is not recommended to be performed actively because it is painful under awake conditions
Evaluation by otolaryngology for the nasal septum and paranasal sinuses, exclusion of intracranial complications by neurosurgery, and planning of skeletal reduction by plastic surgery are necessary.
Le Fort fracture: More extensive facial bone fracture, accompanied by malocclusion and instability of the midface
Nasoethmoid fracture: Accompanied by nasal root depression and medial canthal ligament rupture
Isolated zygomatic arch fracture: Isolated fracture of the zygomatic arch without orbital floor fracture
QWhat other tests are needed besides CT?
A
In addition to CT imaging, functional evaluation of eye movements (Hess chart, binocular single vision test) is important. The forced duction test is used to confirm extraocular muscle entrapment, but imaging and clinical findings are often sufficient for diagnosis. Furthermore, collaboration with otolaryngology, plastic surgery, and neurosurgery is necessary to comprehensively assess intracranial complications, sinus damage, and the need for skeletal reduction.
Performed under general anesthesia. The orbital rim periosteum is approached percutaneously (via subciliary skin incision) or transconjunctivally (via inferior fornix conjunctival incision), and all herniated soft tissues are reduced back into the orbit. After reduction, a forced duction test is performed to confirm release of entrapment.
Fracture repair is performed using bone fragments when possible; for comminuted fractures, the orbital floor is reconstructed using a silicone plate or absorbable plate (made of poly-L/D-lactic acid).
In skeletal reduction performed by otolaryngology or plastic surgery, the entire zygomatic bone is elevated to its normal position and fixed with plates and screws. Main approaches include the Gillies method (elevation of the zygomatic arch via a temporal incision) and direct plate fixation under visualization.
No nose blowing: Avoid blowing the nose for 4–6 weeks postoperatively (to prevent worsening of orbital emphysema).
Monitoring of eye movements: Regularly assessed using the Hess chart.
Antibiotics: Perioperative prophylactic administration such as amoxicillin/clavulanate is used.
Steroids: Short-term administration (prednisone 0.75–1.0 mg/kg/day for 3–5 days) may be given to reduce edema.
QIs ZMC fracture surgery performed by ophthalmology?
A
ZMC fracture surgery is performed collaboratively by multiple departments. Skeletal reduction of the entire zygomatic bone (plate fixation and zygomatic arch elevation) is primarily handled by plastic surgery or otolaryngology. Ophthalmology is responsible for orbital floor fracture reduction and reconstruction, as well as eye protection. Neurosurgery is involved when there are intracranial complications. The division of roles varies depending on each institution’s specialty setup, but it is rare for a single department to handle it alone; a team approach is fundamental.
6. Pathophysiology and Detailed Mechanism of Onset
The zygomatic bone is located in the prominent part of the face and articulates with four bones via sutures and joints. These four junctions can be weak points against external forces.
Frontozygomatic suture: Suture between the zygomatic bone and frontal bone (superolateral angle of the orbit)
Zygomaticomaxillary suture: Suture between the zygomatic bone and maxilla (corresponding to the infraorbital margin)
Zygomatic arch: An arch-like structure extending posteriorly from the zygomatic bone to articulate with the temporal bone
Orbital floor (zygomatic orbital part): Forms the lateral part of the orbital floor
When a direct external force is applied to the cheek area, the zygomatic bone is simultaneously separated at the four sutures and displaced (depressed) medially and inferiorly. This leads to a chain of changes:
Orbital floor fracture: The orbital floor fractures as the zygomatic bone is pushed downward
Orbital content herniation: Orbital fat and, in some cases, the inferior rectus muscle herniate into the maxillary sinus through the fracture site
Orbital volume expansion: Herniation of orbital contents increases the effective orbital volume, causing the eyeball to move posteriorly, resulting in enophthalmos
Infraorbital nerve injury: The infraorbital nerve (second branch of the trigeminal nerve) running in the infraorbital groove is damaged at the fracture site, causing sensory disturbance from the cheek to the upper lip
When the zygomatic arch is depressed, the bone fragment interferes with the coronoid process of the mandible (attachment of the temporalis muscle) and the temporalis and masseter muscles. This mechanically impedes mouth opening, leading to trismus and pain on opening.
Within the orbit, there are septa (orbital septa) running through the orbital fat. Even if only the septum near an extraocular muscle is caught at the fracture site, eye movement restriction can occur. In particular, entrapment of the inferior rectus muscle can cause vertical diplopia and may trigger the oculocardiac reflex (vagal reflex). In young people and children, because the bone is more elastic, a closed (trapdoor) fracture is more likely to occur, where the bone fragment returns to its original position, posing a risk of the extraocular muscle being pinched in the fracture site. In such cases, there is a risk of muscle necrosis, and emergency surgery within 24 hours is necessary.
Miran B, Toneatti DJ, Schaller B, Kalaitsidou I. Management Strategies for Isolated Orbital Floor Fractures: A Systematic Review of Clinical Outcomes and Surgical Approaches. Diagnostics (Basel, Switzerland). 2025;15(23). doi:10.3390/diagnostics15233024. PMID:41374405; PMCID:PMC12690994.
Sivam A, Enninghorst N. The Dilemma of Reconstructive Material Choice for Orbital Floor Fracture: A Narrative Review. Medicines (Basel, Switzerland). 2022;9(1). doi:10.3390/medicines9010006. PMID:35049939; PMCID:PMC8778999.
de Santana IHG, Viana MRM, Palhano-Dias JC, Ferreira-Júnior O, Sant’Ana E, Shinohara ÉH, et al. Orbital floor fracture (blow out) and its repercussions on eye movement: a systematic review. European journal of medical research. 2024;29(1):427. doi:10.1186/s40001-024-02023-y. PMID:39164786; PMCID:PMC11334373.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.