Duane Syndrome (Duane Retraction Syndrome, DRS) is a congenital, non-progressive strabismus syndrome first detailed by Alexander Duane in 1905. Also known as Stilling-Türk-Duane syndrome, it is classified under ICD-10 code H50.81. It is a congenital eye movement disorder characterized by severe abduction limitation and retraction of the eyeball with narrowing of the palpebral fissure on adduction.
It occurs in approximately 1 in 1,000 people in the general population2) and accounts for up to 4% of all strabismus cases. It is the most common congenital cranial dysinnervation disorder (CCDD)2). Unilateral involvement occurs in 82% of cases, more commonly in the left eye (59%), with a female predominance (female-to-male ratio 4:6). Bilateral involvement is seen in 15–20% of cases. Most cases are diagnosed by age 10.
Features: Abduction limitation > adduction limitation. May present with esotropia in primary gaze.
Head posture: Most commonly face turn toward the affected side. 72% have face turn (68% toward the affected side) 1)
MRI findings: The abducens nerve is absent in about 80% of cases.
Epidemiology: Anvari (125 cases) reported Type I in 87.0% 1)
Types II and III
Type II (5–10%): Adduction limitation > abduction limitation. Presents with exotropia in primary gaze and face turn opposite to Type I. MRI shows the abducens nerve is present in most cases.
Type III (10–20%): Both abduction and adduction are limited. 93% have face turn (73% opposite to the affected side) 1)
In a large study (441 patients), facial turn was observed in 54.6%, and the frequency of facial turn was significantly higher in unilateral cases1). Horizontal deviation was 76.0%, esotropia 58.4%, and exotropia 17.6%1).
QHow common is Duane syndrome?
A
It occurs in about 1 in 1,000 people in the general population2) and accounts for up to 4% of all strabismus. It is the most common congenital cranial dysinnervation disorder (CCDD). Unilateral cases account for 82%, with a slight predominance in the left eye and in girls. Most are diagnosed by age 10.
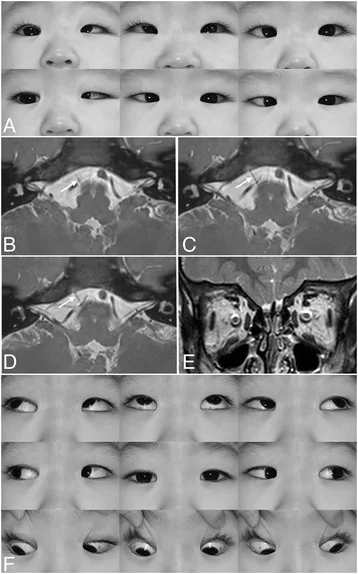
Kim JH, et al. Postoperative full abduction in a patient of Duane retraction syndrome without an abducens nerve: a case report. BMC Ophthalmol. 2017. Figure 1. PMCID: PMC5438545. License: CC BY.
Multi-directional gaze in left Duane syndrome: left eye shows abduction limitation, palpebral fissure narrowing on adduction, and mild upshoot. These correspond to the characteristic eye movement abnormalities discussed in the section “Main Symptoms and Clinical Findings.”
Binocular vision: In most cases, binocular vision is normal, and visual impairment is rare.
Compensatory head turn: The patient maintains binocular vision by turning the face toward the affected side to compensate for abduction deficit. It is necessary to thoroughly explain to parents and teachers that this abnormal head posture is a necessary action to compensate for eye movement disorder and enable binocular vision.
Amblyopia: Occurs in about 10% of cases but responds well to standard treatment. A study of 78 patients in Korea reported amblyopia in 5.1%1).
Refractive error: Hyperopia is the most common. Hyperopia 42.3% and myopia 39.7% have been reported1). Since refractive errors often coexist, treatment for anisometropic amblyopia may be necessary.
Abduction limitation: Complete or partial limitation of abduction (degree varies by type).
Globe retraction + palpebral fissure narrowing: The eye retracts and the palpebral fissure narrows on adduction (induced ptosis). This is a characteristic finding of DRS and is easier to confirm when observed from the side. If fissure narrowing is not clearly seen during adduction, observing the eye from the side while adducting makes globe retraction more noticeable.
Palpebral fissure widening: The palpebral fissure widens on abduction.
Up-shoot/down-shoot (leash phenomenon): The eye deviates upward or downward on adduction. This is not present at birth but occurs secondarily due to progressive contracture of the lateral rectus muscle. If the lateral rectus muscle shifts upward during adduction, an up-shoot occurs; if it shifts downward, a down-shoot occurs.
30–50% of patients have abnormalities due to congenital brainstem disorders. Examples include crocodile tears (gustatory lacrimation) and sensorineural hearing loss.
Related syndromes include Duane radial ray syndrome (SALL4 mutation), Goldenhar syndrome, and HOXA1 syndrome 2).
QDoes compensatory face turn require treatment?
A
Compensatory head turn is an adaptive movement to maintain binocular vision. If the turn is mild (less than 15°), observation without treatment is the standard. Surgery is considered when the turn is 15° or more, or when it causes problems in daily life or cosmesis. Environmental adjustments, such as seating the child in the direction they turn their face at school, are also effective.
Abducens nerve (CN6) deficiency: Damage during the 4th to 8th week of embryonic development leads to absence or hypoplasia of abducens nerve motor neurons. The abducens nucleus and nerve on the affected side of the brainstem are hypoplastic or absent.
Abnormal innervation by the oculomotor nerve (CN3): The adductor branch of CN3 abnormally innervates the lateral rectus muscle, causing simultaneous contraction of the medial and lateral rectus muscles during adduction, leading to globe retraction. Narrowing of the palpebral fissure occurs passively due to globe retraction.
Changes in the lateral rectus muscle: Histologically, a portion of the lateral rectus muscle (the part not receiving normal innervation) becomes fibrotic.
10% of isolated cases are hereditary. 90% are sporadic. Type I is reported as autosomal dominant (8q13), and Type II as autosomal dominant (DURS2: CHN1 mutation, 2q31-q32.1). The following major gene mutations have been reported 2).
CHN1 mutation: Missense mutation in α2-chimaerin (Rac-GAP protein). The residues maintaining the closed conformation of the protein are disrupted, leading to excessive RacGAP activity. CHN1 mutations often result in bilateral DRS and may also involve vertical abnormalities.
MAFB mutation: Heterozygous loss-of-function mutation causing sporadic DRS. Some cases present with DRS plus hearing loss and focal segmental glomerulosclerosis (FSGS).
SALL4 mutation: Duane radial ray syndrome (DRS plus upper limb malformation), autosomal dominant.
Slit lamp and eye movement examination: Globe retraction and narrowing of the palpebral fissure on adduction are characteristic of DRS. Observing from the side makes it easier to confirm globe retraction.
Forced duction test: Positive (central but with contractile changes in extraocular muscles). Useful for differentiating mechanical restriction from innervational deficit.
MRI: Can detect absence or hypoplasia of the abducens nerve. In 80% of type I, MRI shows absence of the abducens nerve, whereas in most type II cases, the abducens nerve is present. Not recommended for routine diagnosis but useful for preoperative evaluation.
Genetic testing (CHN1): Recommended only for familial cases.
Refractive correction (glasses): In some cases, correction of hyperopia alone eliminates face turn and esotropia1). Priority is given to treating refractive errors and anisometropic amblyopia.
Amblyopia treatment: If amblyopia is present, standard occlusion therapy is performed. In many Duane syndrome cases, binocular vision is achieved through face turn, so the risk of strabismic amblyopia is not high.
Botulinum toxin injection: In a study of 25 patients by Anand, abnormal head posture (AHP) improved from 11.58°±7.43° to 7.86°±6.25°1). In 16 patients by Ameri, facial rotation of 18.27°±7.29° improved to 0.094° after one week, but increased again to 7° after six months1).
Surgical indications: Abnormal head posture of 15° or more, significant deviation in primary position, severe induced ptosis (palpebral fissure height reduced by 50% or more).
Esotropic DRS
Medial rectus recession is the basic procedure. It is effective in type I Duane syndrome with strong esotropia or abnormal head posture.
For esotropia less than 15Δ, unilateral medial rectus recession of 6mm can be sufficient. For larger deviations, bilateral medial rectus recession is performed.
Note that recession exceeding 5mm carries risks of adduction limitation and consecutive exotropia.
A combination of the Nishida procedure and medial rectus recession improved esotropia from 40 PD to 6 PD and recovered abduction to 45° in one report1).
Severe/Refractory Cases
For upshoot/downshoot, lateral rectus recession or Y-splitting of the lateral rectus is performed. In any case, complete cure is not achieved, so indications should be determined carefully.
Combined lateral rectus fixation to the periosteum (or large recession) and medial rectus recession is also effective.
Vertical rectus transposition (VRT): The superior and inferior rectus muscles are transposed to the lateral rectus insertion. In the augmented suture group, AHP improved from 22.7° to 3.6°, and in the non-augmented group from 18.7° to 7°1).
QHow effective is botulinum toxin injection?
A
Botulinum toxin temporarily improves abnormal head posture and esotropia, but the effect diminishes after 6 months 1). It is considered as an alternative or adjunct to surgery for early intervention in infancy or in cases with high surgical risk. Repeated injections may be necessary.
QCan surgery cure Duane syndrome?
A
Surgery does not improve the underlying neurological disorder, which is a congenital absence of the abducens nerve and aberrant innervation by the oculomotor nerve. The goals of surgery are to correct deviation in primary position, reduce compensatory head posture, and improve induced ptosis; normalization of eye movement range is not expected. Many patients can maintain good binocular vision postoperatively through compensatory mechanisms.
The current mainstream theory is the neurogenic theory.
Timing of occurrence: Loss of abducens motor neurons occurs during embryonic weeks 4–8. Postmortem anatomical studies at Johns Hopkins University in the 1980s established the neurogenic mechanism.
Mechanism of abnormal innervation: Due to the absence of the abducens nerve, the medial rectus branch of the oculomotor nerve (CN3) abnormally innervates the lateral rectus muscle. During adduction, simultaneous contraction of the medial and lateral rectus muscles occurs, leading to retraction of the eyeball. Narrowing of the palpebral fissure occurs passively due to eyeball retraction.
EMG findings: Absence of electrical activity in the lateral rectus muscle during abduction and paradoxical activation during adduction (first reported in 1956) have been demonstrated.
MRI findings: Absence or hypoplasia of the abducens nerve can be visualized. In type I, 80% show absence; in type II, it is present in most cases.
DRS is a continuum of abnormal innervation phenotypes: There are no strict boundaries between types, and patterns of abnormal innervation are distributed in a diverse manner.
Spatial proximity: The spatial proximity of CN3 and CN6 within the cavernous sinus and orbital apex promotes axonal misdirection.
Myogenic theory (historical): There was a period when fibrosis of the lateral rectus muscle or abnormal posterior attachment of the medial rectus muscle was considered the cause, but this does not adequately explain the paradoxical movement patterns, and the neurogenic theory is now mainstream.
As a primary axonal defect, abnormal innervation of the lateral rectus muscle by CN3 is not due to a primary developmental abnormality of CN3 itself, but rather a secondary phenomenon in which the lateral rectus muscle remains uninnervated due to CN6 deficiency and attracts CN3 axons, as shown in animal models2). MafB is a transcription factor expressed in rhombomeres 5-6 and is not expressed in developing oculomotor motor neurons. Therefore, abnormal branching of CN3 to the lateral rectus muscle is not a cell-autonomous change in CN3 but a secondary phenomenon due to the lack of CN6 innervation2).
In CHN1 knock-in mice, axonal stalling of the abducens nerve occurs, followed by loss of abducens motor neurons. CHN1 mutations involve the pathway in which α2-chimaerin functions as a downstream effector of EphA4 and mediates repulsive signals of ephrin-A52).