Contact lenses (CLs) are highly regulated medical devices worn directly on the cornea. If used without proper care, they can cause serious complications such as corneal infections and corneal ulcers that may have lasting effects on vision.
The number of contact lens wearers is estimated at about 15 to 18 million 1). It has been reported that about 65% of contact lens-related corneal infections are caused by poor care 2), so both the prescriber and the wearer need to understand the care steps and the importance of regular checkups correctly.
The care required depends on the type of contact lens. Daily disposable soft contact lenses are discarded every day, so lens care is not needed 3). Two-week replacement and monthly soft contact lenses require proper daily care. To prevent corneal damage caused by inadequate care, you must follow the instructions for each product.
The two pillars of preventing contact lens-related complications are following the correct care steps and having regular eye examinations. If either is missing, the preventive effect is cut in half.
Disinfection is recommended because of the complex shape
All SCLs need disinfection. HCLs generally do not need disinfection, but for dirt that is hard to remove with routine care, using a dedicated cleaner is recommended. Note that abrasive cleaners cannot be used with some HCLs, so check before use.
For HCL fitting evaluation, confirming the fitting pattern with fluorescein staining is the basic approach. When there is a lot of tearing, it is easy to judge incorrectly, so evaluate after the tearing has settled. SCL fitting evaluation is judged by the push-up test and by checking whether the lens edge rides up onto the cornea when looking up, down, left, and right.
Can clean, rinse, disinfect, and store in one solution
Weak disinfecting effect against fungi and viruses. Rubbing is required
Hydrogen peroxide solutions
They have a stronger disinfecting effect than MPS
If neutralization is incomplete, it can cause corneoconjunctival damage
Povidone-iodine solutions
They have the strongest disinfecting effect
Iodine allergy is a contraindication
Even if the disinfecting effect is increased, neglecting the basic steps of rubbing, rinsing, and cleaning and drying the lens case can cause serious eye damage such as corneal ulcers. Following the correct care steps is far more important than choosing the care solution.
Daily SCL care is performed in the following steps.
① Hand washing: Wash well with soap and dry thoroughly with a paper towel or similar2)
② Rub cleaning: Place the lens in the palm of your hand and rub it with care solution (at least 20 times on each side)2). Even if an MPS label says ‘rinsing only is OK’, do not skip rub cleaning
③ Rinse: Rinse the lens with plenty of care solution2)
④ Soaking in the lens case: Fill a clean lens case with care solution and place the lens in it
⑤ Allow disinfection time: MPS usually requires at least 4 hours (follow the time specified for the product)
The lens case can easily become a breeding ground for biofilm (a film formed by bacteria, Acanthamoeba, and others), and if it is not handled properly, it can become a source of infection when wearing CL4).
After use, discard the care solution, rinse the inside of the case with tap water, then turn it upside down and let it air-dry4)
Replace the lens case with a new one every 3 months4)
SCLs must not be washed or stored in tap water. Tap water contains Acanthamoeba that can survive even chlorination and can cause severe Acanthamoeba keratitis. More than 90% of CL-related Acanthamoeba keratitis occurs in contact lens wearers, and contact with tap water is considered the main route of infection4). Rinsing HCLs is also recommended to be done with a dedicated care solution or saline.
Importance of regular checkups and visit intervals
Regular checkups are essential for early detection of early corneal damage without symptoms. Many contact lens wearers do not visit an eye clinic until they start to feel discomfort, but by then complications may already have progressed.
Visual acuity and refraction measurement: evaluation of refractive fluctuation and whether the lens power is appropriate
Check for corneal and conjunctival complications: early detection of corneal epithelial damage (SPK), corneal vascularization, giant papillary conjunctivitis (GPC), and corneal infection
Lens condition check: assessment of scratches, contamination, and deformation
Fitting assessment: check lens movement while worn and lens edge position
Visit at 1 week, 1 month, and 3 months after starting wear5)
Stable wearers
At least once a year (every 6–12 months)5)
When problems occur
Same-day visit
The contact lens clinical guidelines recommend at least one visit per year even for stable wearers5). New wearers should have closely spaced visits during the first 3 months to check fitting and whether any complications are present early.
QHow often should regular contact lens checkups be done?
A
For stable wearers, at least one visit per year is recommended5). New wearers should be seen at 1 week, 1 month, and 3 months after starting wear to check fitting and whether complications are present. Even without symptoms, corneal neovascularization and corneal epithelial damage can progress, so regular visits should not be skipped. Also, if there is a prescription change (a change in eyeglasses or contact lens power) or any trouble such as eye redness, pain, or blurred vision, prompt medical attention is needed.
5. Main complications associated with contact lens wear and how to manage them
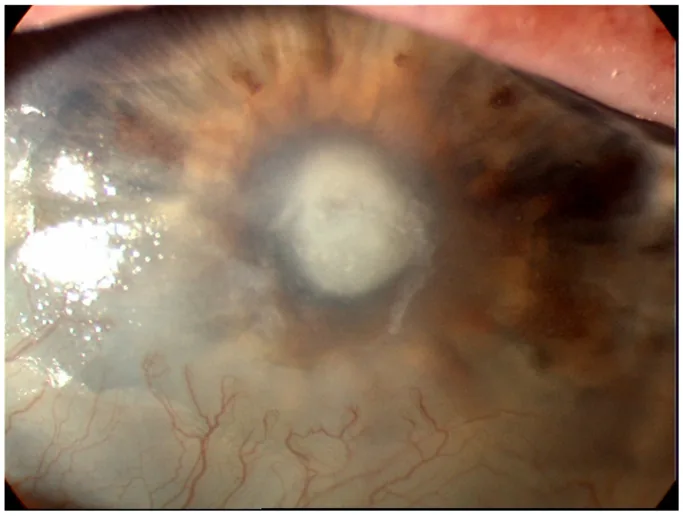
Tanhapour M, et al. Corneal Ulceration in Bacterial Keratitis. Diagnostics (Basel). 2023;13(21):3358. Figure 1. PMCID: PMC10647798. License: CC BY 4.0.
In the slit-lamp photograph, a white stromal infiltrate at the center of the cornea and an ulcer base with an epithelial defect can be seen. This corresponds to the bacterial keratitis discussed in the section on main complications associated with contact lens wear and how to manage them.
Causative organisms: mainly Pseudomonas aeruginosa, Staphylococcus species, and others2)
Features: It progresses rapidly and forms a corneal ulcer. Without proper antibiotic eye drop treatment, visual impairment can remain.
Prevention: rubbing and rinsing, proper lens case care, and avoiding overnight wear
Acanthamoeba keratitis
Cause: More than 90% of cases occur in contact lens wearers. Using tap water and wearing lenses around water are the main risk factors4)
Features: Causes severe eye pain, and in the early stage it is hard to distinguish from bacterial or viral infection. It is highly resistant to treatment
Prevention: Completely avoid contact with tap water. Do not bathe or swim while wearing contact lenses
Fungal keratitis
Reports: Outbreaks of Fusarium species infections have been reported in MPS users6)
Features: Progresses slowly and is often diagnosed late. Antifungal treatment is needed
Prevention: Strictly follow care procedures. Replace the lens case regularly
Other complications
Corneal vascular ingrowth: New blood vessel growth caused by low oxygen. Consider switching to a lens with high oxygen permeability (Dk/t)
Giant papillary conjunctivitis (GPC): Papillary proliferation of the upper eyelid conjunctiva. Consider changing the type of lens and using antiallergy eye drops
Corneal epithelial damage (SPK): Shorten wearing time and use artificial tears
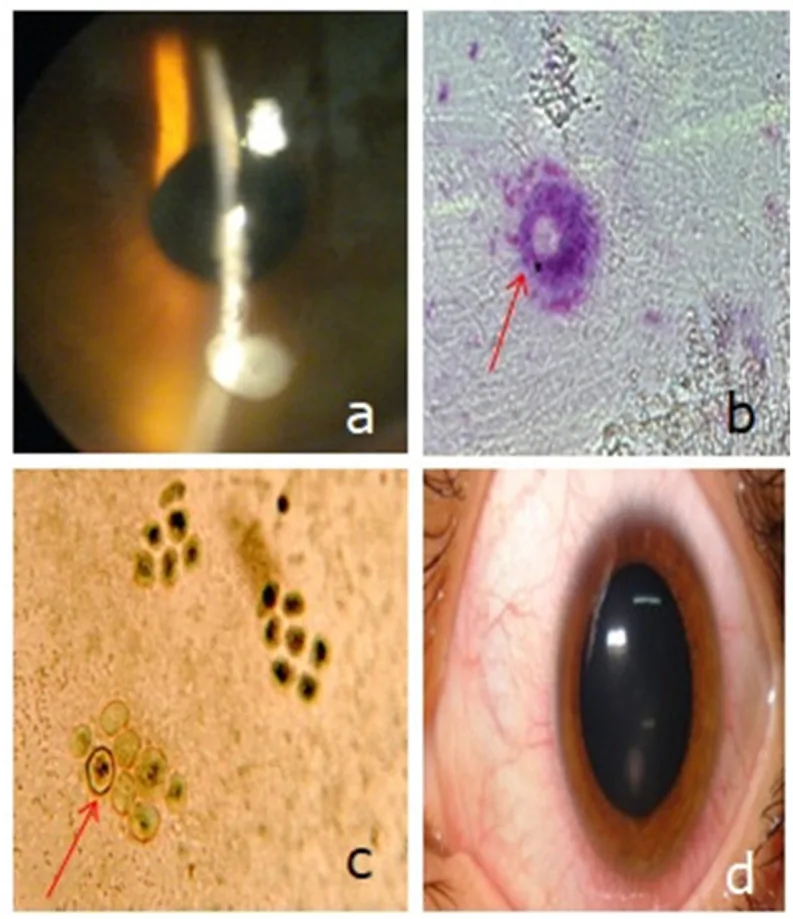
Nadia BA, Anis M, Ali SM, et al. Acanthamoeba keratitis in contact lens wearers in a tertiary center of Tunisia, North Africa. Ann Med Surg (Lond). 2021;70:102834. Figure 3. PMID: 34567549; PMCID: PMC8449026; DOI: 10.1016/j.amsu.2021.102834. License: CC BY 4.0.
Anterior segment photograph of a monthly disposable soft CL wearer showing Acanthamoeba keratitis with infiltrates extending into the corneal stroma. Corresponds to the Acanthamoeba keratitis covered in the section on major complications associated with CL wear and how to manage them.
CL wear can increase tear evaporation and destabilize the tear film, contributing to the onset and worsening of dry eye7). The combination with long periods of screen use is especially hard on the tear film. CL-compatible artificial tears (without benzalkonium chloride: BAK-free) are recommended.
After surgery (after cataract surgery, after LASIK, etc.): Resume wearing only after getting approval from your doctor. It may take time for the corneal condition to stabilize after surgery.
Allergic conditions: During times when allergies worsen, such as during pollen season, daily disposable lenses are recommended.
During pregnancy: Hormonal changes may alter your refraction. Your prescription may need to be adjusted.
The use of silicone hydrogel (SiHy) contact lenses, which have high oxygen permeability, is increasing. SiHy materials are designed to reduce the cornea’s oxygen deprivation load, and deciding whether they are appropriate for each case is important.
Research is advancing on smart contact lenses equipped with eye pressure sensors and blood glucose monitoring functions9). Contact lens applications are expected for managing intraocular pressure in glaucoma and monitoring glucose in people with diabetes, but they are not yet in clinical use.
Development of antibacterial-coated contact lenses
Research is progressing on infection-prevention technologies that coat contact lens surfaces with antimicrobial substances9). The goal is to further reduce the rate of contact lens-related infections through surface treatments that inhibit biofilm formation and through the application of nanomaterials.
Research is progressing on optimizing contact lens fitting using corneal shape analysis with artificial intelligence (AI). A system that supports precise contact lens prescribing tailored to each person’s corneal shape is expected to become practical.
Stapleton F, Keay L, Edwards K, Naduvilath T, Dart JK, Brian G, et al. The incidence of contact lens-related microbial keratitis in Australia. Ophthalmology. 2008;115(10):1655-62. doi:10.1016/j.ophtha.2008.04.002. PMID:18538404.
Morgan PB, Efron N. A decade of contact lens prescribing trends in the United Kingdom (1996-2005). Cont Lens Anterior Eye. 2006;29(2):59-68. doi:10.1016/j.clae.2006.02.008.
Joslin CE, Tu EY, McMahon TT, Passaro DJ, Stayner LT, Sugar J. Epidemiological characteristics of a Chicago-area Acanthamoeba keratitis outbreak. American journal of ophthalmology. 2006;142(2):212-7. doi:10.1016/j.ajo.2006.04.034. PMID:16876498.
Chang DC, Grant GB, O’Donnell K, Wannemuehler KA, Noble-Wang J, Rao CY, et al. Multistate outbreak of Fusarium keratitis associated with use of a contact lens solution. JAMA. 2006;296(8):953-63. doi:10.1001/jama.296.8.953. PMID:16926355.
Nichols JJ, Willcox MD, Bron AJ, Belmonte C, Ciolino JB, Craig JP, et al. The TFOS International Workshop on Contact Lens Discomfort: executive summary. Investigative ophthalmology & visual science. 2013;54(11):TFOS7-TFOS13. doi:10.1167/iovs.13-13212. PMID:24058135; PMCID:PMC4686219.
Schein OD, McNally JJ, Katz J, Chalmers RL, Tielsch JM, Alfonso E, et al. The incidence of microbial keratitis among wearers of a 30-day silicone hydrogel extended-wear contact lens. Ophthalmology. 2005;112(12):2172-9. doi:10.1016/j.ophtha.2005.09.014. PMID:16325711.
Farandos NM, Yetisen AK, Monteiro MJ, et al. Contact lens sensors in ocular diagnostics. Adv Healthc Mater. 2015;4(6):792-810. doi:10.1002/adhm.201400504.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.