Raymond syndrome is an alternating hemiplegia syndrome caused by a lesion in the ventromedial mid-pons. It was first reported in 1895 by French neurologist Fulgence Raymond. The case involved a 39-year-old woman with syphilis who presented with a triad of abducens nerve palsy, contralateral facial nerve palsy, and hemiplegia, suggesting a lesion at the crossing of facial nerve fibers in the caudal medial pons1).
Since the initial report, only a few cases of pure Raymond syndrome have been documented in the literature, making it an extremely rare condition2,3). Recent case reports have discussed the validity of classifying it into two types: the classic type (with facial nerve palsy) and the common type (sparing the face)1,4).
Contralateral central facial nerve palsy: Due to damage to the corticofacial fibers that cross at the pontine level. Only the lower face is paralyzed, while forehead wrinkling is preserved.
Contralateral hemiplegia: Due to damage to the corticospinal tract. The classic type is rarer than the common type.
Contralateral hemiparesis: due to lesion of the corticospinal tract. No facial nerve palsy.
The corticofacial fibers running dorsally are not affected by the ventral pontine lesion, resulting in facial sparing.
Related brainstem syndromes to be aware of for differential diagnosis:
Millard-Gubler syndrome: ipsilateral abducens nerve palsy and contralateral hemiparesis (similar to common type of Raymond syndrome). It differs by the presence of peripheral facial nerve palsy due to direct involvement of the facial nerve nucleus.
Foville syndrome: Pontine lesion presenting with conjugate gaze palsy toward the lesion side, facial nerve palsy, taste loss, Horner syndrome, and hearing loss.
QHow is Raymond syndrome different from Millard-Gubler syndrome?
A
Millard-Gubler syndrome presents with abducens nerve palsy and contralateral hemiplegia, similar to the common type of Raymond syndrome, but differs in that it involves peripheral facial nerve palsy due to direct damage to the facial nerve nucleus (affecting forehead wrinkling as well). In the classic type of Raymond syndrome, facial nerve palsy is central due to damage to the corticofacial fibers below the nucleus, affecting only the lower face.
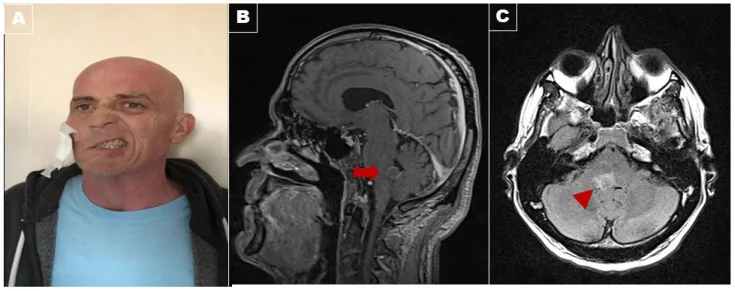
A Rare Neuro-Ophthalmological Condition in a Patient with Lung Adenocarcinoma: The Eight-and-a-Half Syndrome, Case Report and Review of the Literature. Brain Sci. 2022 Mar 28; 12(4):451. Figure 1. PMCID: PMC9030817. License: CC BY.
Panel (A): The patient showed severe right facial palsy with a peripheral pattern with Bell’s sign, rightward conjugate gaze palsy, and right internuclear ophthalmoplegia. The leftward gaze evoked left-beating nystagmus. Postcontrast T1-weighted Magnetic resonance imaging in the sagittal view (Panel (B)) demonstrated a ring enhancement lesion (arrow) on fluid-attenuated inversion recovery (FLAIR) in the axial view (arrowhead; Panel (C)) in the dorsal tegmentum of the pons, suggestive of metastasis.
Abnormal head posture: Face turn toward the paretic eye to reduce diplopia.
Unilateral limb weakness: Due to contralateral hemiparesis.
Abnormal facial movements (classic type only): Motor impairment of the lower face, such as drooping of the mouth corner, due to contralateral central facial nerve palsy.
Clinical Findings (Findings Confirmed by Physician Examination)
Ipsilateral abducens nerve palsy: Limited abduction of the affected eye. Confirmed by cover test and Hess chart, showing a pattern contraction in the abduction direction of the affected eye on primary deviation.
Contralateral hemiparesis: Motor impairment of the contralateral upper and lower limbs due to damage to the corticospinal tract.
Contralateral central facial nerve palsy (classic type only): Paralysis only of the lower face, with forehead wrinkling preserved.
QHow do symptoms differ between the classic type and the common type?
A
The classic type presents with the triad of abducens nerve palsy, contralateral central facial nerve palsy, and contralateral hemiplegia. The common type does not involve facial nerve palsy and shows only the two signs of abducens nerve palsy and contralateral hemiplegia. The classic type is much rarer than the common type.
Raymond syndrome is caused by a lesion in the medial ventral caudal pons.
Pontine infarction: The most common cause. Most cases are due to small vessel disease 3,5).
Lacunar infarction: Small infarction due to occlusion of pontine perforating arteries. Typical cases involve occlusion of the basilar artery paramedian branches 5).
Hemorrhage from a cavernous hemangioma at the pontomedullary junction: A reported cause 2).
The greatest risk factor is hypertension, and almost all reported cases mention the involvement of hypertension. Diabetes and hyperlipidemia, which are risk factors for arteriosclerosis, are also important as underlying conditions.
As a common cause of isolated abducens nerve palsy, ischemic (small vessel disease due to hypertension and diabetes) is most common in people over 50, and it often resolves spontaneously within 3 to 6 months.
Raymond syndrome has no clearly defined diagnostic criteria. Diagnosis is made by a combination of imaging and clinical findings.
Essential clinical signs are the combination of abducens nerve palsy and contralateral hemiplegia; contralateral facial nerve palsy is rare (classic type only).
Diffusion-weighted imaging (DWI): May show cytotoxic edema in the ventromedial portion of the mid-pons. Infarct can be detected as a hyperintense signal from the hyperacute phase (within 1–3 hours of onset).
FLAIR imaging: Shows hyperintense signal from approximately 3–6 hours after onset.
Treatment of the underlying disease is the first priority.
Thrombolytic therapy (tPA intravenous injection): Considered within 4.5 hours of symptom onset if no contraindications. It may be indicated if an infarct is confirmed on MRI diffusion-weighted imaging within 4.5 hours of onset.
Neuroprotective drugs: Edaravone (Radicut®) intravenous drip infusion is an option within 24 hours of onset.
Conservative observation: For isolated ocular motor abnormalities, ultra-acute treatment is rarely performed; observation with Mecobalamin® tablets 500 μg 3 tablets and Kallikrein® tablets 10 units 3 tablets (each divided into 3 doses) is common (both are off-label).
Treatment for Abducens Nerve Palsy (Chronic Phase / Residual Palsy)
Considered if no improvement after 6 months and diplopia is severe.
Mild to moderate palsy (able to cross midline on abduction): Lateral rectus resection and medial rectus recession.
Severe palsy (unable to cross midline): Vertical rectus transposition (muscle transposition). Recently, minimally invasive full vertical rectus transposition has been developed, with good reported outcomes for eye alignment.
The purpose of surgery is not to resolve the paralysis but to reduce symptoms by adjusting muscle tension balance. Explain thoroughly to the patient that residual diplopia on lateral gaze is inevitable after surgery.
QHow long does it take for diplopia due to abducens nerve palsy to improve?
A
Cases caused by peripheral circulatory disorders (small vessel disease due to hypertension or diabetes) often improve spontaneously within 3 to 6 months. If there is no improvement after 6 months and diplopia is severe, extraocular muscle surgery is considered. Recovery is influenced by the function at onset, age, and the status of rehabilitation.
6. Pathophysiology and Detailed Mechanism of Onset
Abducens nucleus: Located in the dorsal pons, protruding into the floor of the fourth ventricle.
Large cells: Send efferent nerve fibers that innervate the ipsilateral lateral rectus muscle.
Small cells (internuclear neurons): Send internuclear fibers (medial longitudinal fasciculus, MLF) to the contralateral oculomotor medial rectus subnucleus, controlling conjugate horizontal eye movements.
Abducens nerve fiber bundle: Runs ventrally and caudally through the pons, exits the brainstem at the pontomedullary junction without decussating.
Damage to the abducens nucleus causes ipsilateral horizontal conjugate gaze palsy, whereas damage to the abducens nerve fiber bundle causes ipsilateral abducens nerve palsy (infranuclear). Raymond syndrome is the latter.
Damage to the corticospinal tract → Contralateral hemiparesis (the corticospinal tract runs ventrally in the pons and decussates below the pontine level)
Damage to uncrossed corticofacial fibers → Contralateral central facial palsy (classic type only)
Mechanism of presence or absence of facial nerve palsy
Corticofacial fibers pass through multiple pathways, including the aberrant bundle near the medial lemniscus in the pontine tegmentum. Corticofacial fibers running dorsally are not affected by ventral pontine lesions, resulting in facial sparing. Classic contralateral facial palsy occurs only when the lesion involves the decussation of corticofacial fibers at the level of the abducens nerve 4). Ogawa et al. pointed out that some supracore fibers of the corticofacial tract may pass through the aberrant pyramidal tract adjacent to the pyramidal tract, and they suggest that preservation of this fiber bundle is the anatomical basis for the common type (facial-sparing type) 3).
Because many nuclei and fibers are densely packed near the abducens nerve root, it is anatomically difficult for a ventral pontine lesion to selectively damage only the abducens nerve fascicle and corticospinal tract. Therefore, mixed types such as Millard-Gubler syndrome or horizontal gaze palsy are more common, and pure Raymond syndrome cases are extremely rare 1,4,5).
Zaorsky NG, Luo JJ. A case of classic Raymond syndrome. Case Rep Neurol Med. 2012;2012:583123. doi:10.1155/2012/583123. PMID: 22934209; PMCID: PMC3423663.
Satake M, Kira J, Yamada T, Kobayashi T. Raymond syndrome (alternating abducent hemiplegia) caused by a small haematoma at the medial pontomedullary junction. J Neurol Neurosurg Psychiatry. 1995;58(2):261. doi:10.1136/jnnp.58.2.261. PMID: 7876876; PMCID: PMC1073342.
Ogawa K, Suzuki Y, Kamei S. Two patients with abducens nerve palsy and crossed hemiplegia (Raymond syndrome). Acta Neurol Belg. 2010;110(3):270-271. PMID: 21114137.
Mégevand P, Pilly B, Delavelle J, et al. Sixth cranial nerve palsy and contralateral hemiparesis (Raymond’s syndrome) sparing the face. J Neurol. 2009;256(6):1017-1018. doi:10.1007/s00415-009-5041-6. PMID: 19252793.
Ground M, Punter MNM, Rosemergy I. Pontine ischaemic stroke syndromes. Pract Neurol. 2023;23(6):501-503. doi:10.1136/pn-2023-003782. PMID: 37524438.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.