Ocular neuromyotonia (ONM) is a rare eye movement disorder characterized by intermittent and sustained tonic spasms in one or more extraocular muscles. It causes recurrent episodes of paroxysmal strabismus and diplopia. The mechanism is thought to involve involuntary neural discharges from damaged nerves and delayed muscle relaxation.
Most cases are unilateral and occur primarily in adults. The oculomotor nerve (CN III) or abducens nerve (CN VI) is most commonly affected. Typical cases develop after radiation therapy for tumors in the sellar or parasellar region, with onset ranging from 2 months to 18 years after irradiation 1).
Non-radiation-induced ONM is rare but can occur in patients without a history of radiation exposure. Cases triggered by peribulbar block have also been reported 1).
QWho is most likely to develop ocular neuromyotonia?
A
It most commonly occurs in adults with a history of radiation therapy, mainly after treatment for sellar or parasellar tumors (e.g., pituitary tumors). It is usually unilateral and can appear from months to 18 years after irradiation 1).
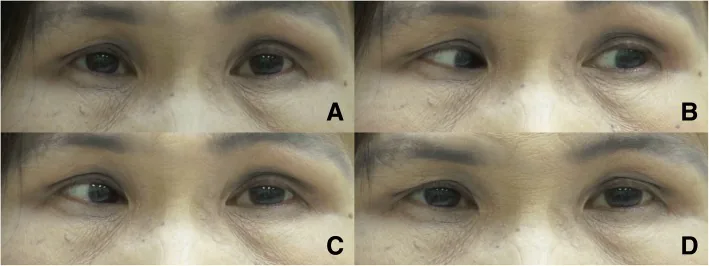
Bilateral oculomotor ocular neuromyotonia: a case report. BMC Neurol. 2018 Sep 3; 18:137. Figure 2. PMCID: PMC6120096. License: CC BY.
Right oculomotor ocular neuromyotonia. The primary position was characterized by orthotropia (a). Following 30 s of left eccentric gaze (b), the patient developed involuntary contraction of the right medial rectus, which resulted in right esotropia while returning both eyes to the primary position (c). The right esotropia lasted approximately 2 min, then spontaneously resolved (d)
Paroxysmal diplopia: Transient double vision that occurs spontaneously or after lateral gaze (deviated eye position).
Duration of episodes: Episodes last from seconds to minutes.
May not be reproduced during examination: Because symptoms are intermittent, an attack may not be observed at the time of the visit.
In a case after retrobulbar block (Zhang 2025), a man in his 60s developed intermittent vertical diplopia several weeks after left eye pterygium surgery. Symptoms were more noticeable in the morning and evening, occurred sporadically during the day (especially while driving), and had been stable since onset1).
Clinical Findings (Findings Confirmed by Physician Examination)
Gaze-evoked ocular fixation: After looking in the direction of action of the affected muscle, the eye becomes stuck in that position. Attempting to return to primary position induces spasm or persistent diplopia.
Sustained gaze test: Can be induced by eccentric gaze for about 10 seconds, and is key to diagnosis.
Absence of eye movement limitation or fatiguability: No limitation of duction (monocular movement) or fatiguability is observed.
Variability in strabismus angle: Some patients may be orthophoric at near but show intermittent strabismus increasing up to 25Δ at distance 1).
QHow is an attack of ocular neuromyotonia confirmed?
A
When the patient gazes in the direction of action of the affected muscle for several seconds to 10 seconds, the eye becomes fixed, and attempting to return to the primary position induces spasm and diplopia. This “gaze-evoked ocular fixation” is key to clinical diagnosis.
In vertical strabismus after peribulbar block, the risk of inferior rectus muscle injury is involved. Needle injury from local anesthesia and/or local anesthetic affecting nerve fibers innervating the extraocular muscles may cause ephaptic transmission.
ONM can be diagnosed clinically. The basis is a careful history and a thorough ocular motor examination observing the eyes in primary position and after a few seconds of lateral gaze.
Prolonged gaze-evoked test: Have the patient gaze in the direction of action of the affected muscle for about 10 seconds. If gaze-evoked nystagmus is confirmed, it strongly supports the diagnosis.
Brain MRI (with gadolinium contrast): Performed to rule out secondary causes. Evaluate for tumors, vascular lesions, and demyelinating lesions 1).
Thyroid function tests: Recommended to rule out underlying thyroid dysfunction.
Others: Electromyography, electrooculography, video recording of eye movements, and muscle biopsy can further analyze the spasms.
Membrane-stabilizing drugs are the standard treatment.
Carbamazepine (first-line drug): Interacts with channels on the nerve membrane, reducing the firing frequency of action potentials and decreasing ephaptic transmission. Start at 100 mg twice daily and adjust according to symptoms1).
Gabapentin, Phenytoin: Membrane-stabilizing mechanism similar to carbamazepine. Used as alternative drugs.
Lacosamide: Alternative for patients who experienced side effects with carbamazepine. Low risk of cross-reactivity and fewer side effects.
Vitamin supplementation: If caused by vitamin B12 or D deficiency, symptoms may resolve after supplementation.
Fresnel prism: Used as symptomatic treatment for diplopia. Can be combined with drug therapy1).
Check liver function, kidney function, and complete blood count at treatment initiation and at 6-week follow-up.
Surgery is considered in cases resistant to drug therapy or when long-term medication is difficult.
Strabismus surgery (recession) : Weakening surgery of the affected muscle. In 7 of 13 reported cases across 7 reports, paroxysmal spasms disappeared after recession surgery1).
Resection/plication (strengthening surgery) : May worsen attacks and is generally avoided.
Microvascular decompression : May be effective in cases caused by vascular compression of the nerve.
In the case by Zhang et al. (2025), a 3.5 mm recession of the left inferior rectus (adjustable suture) was performed, and diplopia markedly improved 4 months postoperatively. Stereopsis of 140 seconds of arc and Worth 4-dot fusion at distance and near were achieved, and no worsening of deviation was observed even in downgaze extension1).
QWill symptoms recur if carbamazepine is stopped?
A
It is known that discontinuing membrane-stabilizing drugs often leads to recurrence1). If side effects are a concern, switching to lacosamide or considering strabismus surgery are options.
The basic mechanism of ONM is ephaptic transmission caused by segmental demyelination of cranial nerves due to radiation injury, compressive diseases, microvascular disorders, etc.
Ephaptic transmission is a phenomenon in which signal crosstalk occurs between adjacent demyelinated nerve fibers, and nerve impulses are transmitted along lateral contacts without synapses. This explains the persistence and repetition of tonic contractions 1).
Other proposed mechanisms are as follows:
Potassium channel dysfunction: Hyperexcitability of the neuronal membrane causes abnormal axonal firing.
Retrograde degeneration and central reorganization: Changes in neural transmission due to denervation and reorganization of motor output patterns in the nerve nucleus are involved.
Reflex neural circuit hypothesis (Eggenberger): Reflection and sprouting axons combine to form an abnormal reflex circuit that amplifies inverted signals.
In thyroid-related orbital disease, inflammatory changes and crowding of the oculomotor nerve and muscle cells cause ONM. Inflammatory cell infiltration of the endomysium and mucopolysaccharide deposition increase nerve excitability, and anti-thyroid peroxidase antibodies may directly induce demyelination.
In ONM after retrobulbar block, needle injury and/or local anesthetics may damage nerve fibers innervating the extraocular muscles, leading to ephaptic transmission. The therapeutic response to carbamazepine supports this hypothesis 1).
QWhy do attacks occur when looking in a specific direction?
A
Ephaptic transmission between demyelinated nerve fibers causes signals from gaze activating a specific muscle to also spread to adjacent damaged nerves, resulting in sustained tonic contraction 1). This is why the eye becomes “fixed.”
Zhang et al.(2025)は、球後局所麻酔後に発症したONMを文献上初めて報告した1)。球後ブロックが新たなONM発症原因として提唱されており、球後ブロック後の垂直斜視例の一部にONMメカニズムが関与している可能性がある。測定値のばらつきとして見逃されている症例が存在すると著者らは指摘している。
Bodi et al. (2024) reported a study on the clinical features, diagnosis, and outcomes of ONM 2). It was shown that spontaneous remission of ONM is rare and long-term management is required.
Prospective studies are difficult to conduct due to the rarity and heterogeneity of vertical strabismus after retrobulbar block, but further investigation is needed to accurately assess the involvement of ONM mechanisms 1).
Zhang JJ, Nguyen MTB, Gaier ED. Ocular neuromyotonia after peribulbar block. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2025;29(1):104096. doi:10.1016/j.jaapos.2024.104096. PMID:39746535; PMCID:PMC11885024.
Bodi TB, Klaehn LD, Kramer AM, Bhatti MT, Brodsky MC, Eggenberger ER, et al. Ocular Neuromyotonia: Clinical Features, Diagnosis, and Outcomes. American journal of ophthalmology. 2024;263:61-69. doi:10.1016/j.ajo.2024.02.003. PMID:38369222.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.