Cryptococcosis is a systemic fungal infection primarily caused by Cryptococcus neoformans and Cryptococcus gattii. When localized in the central nervous system (CNS), it presents as subacute meningoencephalitis and causes various neuro-ophthalmologic signs.
CM is a leading cause of adult meningitis in immunocompromised patients, especially those with HIV infection.
HIV-associated: Accounts for up to 79% of CM cases, with approximately 1 million cases annually. About 700,000 deaths occur each year, with up to 500,000 in sub-Saharan Africa alone. CM accounts for 15–17% of AIDS-related deaths.
HIV-negative individuals: Long-term steroid use (25%), chronic kidney/liver/lung disease (24%), malignancy (16%), solid organ transplant (15%) are background factors. Mortality rate reaches 20–30%.
Immunocompetent individuals: Up to 30% of CM cases occur in immunocompetent individuals without underlying disease, with C. gattii being the most common causative agent.
Reports indicate that mortality exceeds 60% in the first 3 months of infection 5). Even with appropriate antifungal therapy, mortality remains high at 15–30% 5).
QCan cryptococcal meningitis also occur in HIV-negative individuals?
A
Up to 30% of CM cases occur in immunocompetent individuals without underlying disease. In immunocompetent individuals, C. gattii is the main causative agent, and in recent years, patients with anti-GM-CSF autoantibodies have also attracted attention. Mortality in HIV-negative individuals is high at 20–30%.
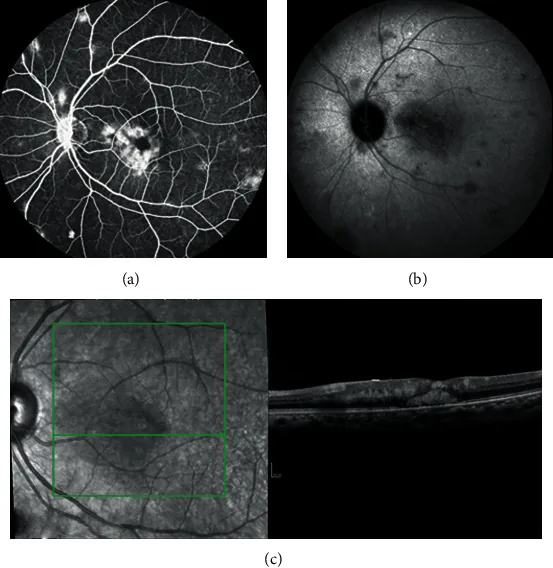
Maria Fernanda Flores Herrera, Nicolas Dauby, Evelyne Maillart et al. Multimodal Imaging in AIDS-Related Ocular Cryptococcosis. Case Reports in Ophthalmological Medicine. 2021 Feb 10; 2021:8894075. Figure 3. PMCID: PMC7892231. License: CC BY.
Neuro-ophthalmic findings in CM can be broadly divided into secondary changes due to elevated ICP and findings from direct infiltration.
Findings due to increased ICP
Papilledema: The most important fundus finding reflecting increased ICP. Often bilateral.
Abducens nerve palsy (CN VI): The most common localized cranial nerve disorder associated with increased ICP. Unilateral or bilateral.
Transient visual obscurations: Temporary visual impairment due to increased ICP.
Findings due to direct infiltration
Optic neuropathy: Direct infiltration of the optic nerve causes vision loss and optic atrophy. The absence of papilledema may help differentiate from increased ICP.
Oculomotor nerve palsy (CN III): Mydriasis, ptosis, and restricted eye movement. Intermittent symptoms due to vasculitis may also occur.
Visual field defects: homonymous hemianopia or quadrantanopia due to optic tract infiltration
Chorioretinitis and endophthalmitis: due to hematogenous dissemination or spread via the pia mater
Granulomatous conjunctivitis and keratitis: rare anterior segment involvement
QWhy does vision loss occur without papilledema?
A
This is due to direct infiltration and destruction of the optic nerve by Cryptococcus. In optic atrophy caused by elevated ICP, papilledema often precedes vision loss, whereas direct infiltration may occur without papilledema. However, this is not a definitive distinguishing feature.
The main causative organisms of CM are the following two species.
C. neoformans: Accounts for approximately 80% of all cases and is distributed worldwide. It primarily infects immunocompromised individuals5)
C. gattii: Can infect immunocompetent individuals and is geographically common in Oceania, western Canada, the Pacific Northwest of the United States, Southeast Asia, and South America
Bird droppings (especially pigeons) and soil in the environment are the main sources of infection, and infection occurs through inhalation of spores5). C. gattii has also been reported to be associated with Eucalyptus trees.
Anti-GM-CSF autoantibodies: A newly recognized risk factor in recent years. Increasingly reported as a cause of disseminated cryptococcosis in patients previously considered immunocompetent6)
CSF pressure measurement: Essential for evaluating ICP elevation. The upper normal limit is considered 25 cmH2O.
CSF findings: Typically show lymphocytic pleocytosis, elevated protein, and low glucose, but in HIV-infected patients, the cellular response may be poor.
Head MRI: Shows dilated Virchow-Robin spaces, gelatinous pseudocysts, meningeal enhancement, and cryptococcomas (granulomatous lesions)1). However, only about 21–27% of cases show typical findings4)
Head CT: Less sensitive than MRI but useful for emergency screening
In HIV-positive individuals, consider initiating antiretroviral therapy (ART) at week 4.
Maintenance Therapy
Fluconazole 200 mg/day, administered daily.
Continue for at least 1 year. In HIV-positive individuals, consider discontinuation if CD4 > 100/uL and viral load undetectable for more than 3 months.
Elevated ICP is a major cause of visual impairment in CM, and aggressive management is essential.
Therapeutic lumbar puncture: performed daily. For high-pressure cases, a maximum of 30 mL per drainage is standard. Most patients achieve adequate control.
CSF shunt surgery (ventriculoperitoneal shunt, lumboperitoneal shunt): considered when management with lumbar puncture is difficult.
Acetazolamide: not recommended. In a randomized controlled trial for CM, serious adverse events occurred more frequently than in the placebo group, leading to early termination of the trial.
It is recommended to delay ART initiation for at least 4 weeks after acute treatment of CM4). Early ART initiation (within 1–2 weeks) increases the risk of immune reconstitution inflammatory syndrome (IRIS) and is associated with increased mortality.
QWhy is acetazolamide not recommended for managing intracranial pressure in CM?
A
A randomized controlled trial in Thailand involving 22 CM patients was terminated early because the acetazolamide group showed a significant decrease in venous bicarbonate levels and an increase in chloride levels, with more frequent serious adverse events than the placebo group. It is recommended to avoid its use whenever possible.
Cryptococcus obstructs the flow of CSF through the arachnoid granulations in the subarachnoid space. Additionally, capsular polysaccharides accumulating in the CSF increase osmotic pressure, causing fluid retention and further elevating ICP. Elevated ICP is the main cause of papilledema and abducens nerve palsy, and the improvement of vision and eye movements with ICP-lowering therapy supports this mechanism.
Histological examination of autopsy cases has confirmed that invasion and destruction of the optic nerve by Cryptococcus is the main cause of optic atrophy. The absence of preceding papilledema in this mechanism may serve as a clinical distinguishing feature.
Infiltration of the optic tract causes homonymous hemianopia or quadrantanopia depending on the site of involvement.
Endarteritis of small branches of the basilar artery and brainstem infarction have been reported in autopsies. This vasculitic mechanism can cause various eye movement disorders.
Internuclear ophthalmoplegia (INO): Due to vascular ischemia of the MLF. Since 1972, only 8 cases of INO/WEBINO (wall-eyed bilateral INO) have been reported, making it extremely rare 1)
Oculomotor nerve disorders: Caused by vasospasm and ischemia, presenting with intermittent symptoms ranging from complete paralysis to isolated mydriasis and ptosis
Cerebral infarction: Ischemic stroke occurs in 13–54% of CM patients, with the basal ganglia, internal capsule, frontal lobe, and thalamus being common sites 1)
Intraocular lesions arise from hematogenous dissemination or extension via the pia mater. Choroiditis, chorioretinitis, vitritis, anterior uveitis, and endophthalmitis have been reported.
C. neoformans crosses the blood-brain barrier via multiple routes: paracellular passage, transcytosis, and infection of monocytes/macrophages (Trojan horse effect) 5). Both C. neoformans and C. gattii exhibit a unique tropism for the brain 5).
QWhy is the abducens nerve most susceptible to damage?
A
The abducens nerve has a long course along the base of the skull, making it anatomically vulnerable to compression due to increased ICP. Therefore, abducens nerve palsy is the most common localizing sign not only in CM but also in various diseases that cause increased intracranial pressure.
7. Latest Research and Future Perspectives (Research Stage Reports)
Solis-Gomez et al. (2025) reported a case of a 53-year-old woman with chronic liver failure in whom internuclear ophthalmoplegia (INO) appeared as the initial symptom of cryptococcal meningitis before initiation of antifungal therapy 1). MRI showed extensive leptomeningeal enhancement and infratentorial nodular enhancement of the midbrain and cerebellar hemispheres, and DWI/ADC confirmed ischemic cerebral infarction. The authors emphasized that intra-axial symptoms including INO can occur due to ischemia mediated by vasculitis, and noted that this was the first reported case of INO preceding treatment. Only 8 cases of INO/WEBINO have been reported since 1972.
Willett et al. (2022) reported a case of endogenous chorioretinitis due to C. gattii in a 37-year-old immunocompetent man 2). The patient presented with a subretinal abscess that progressed to full-thickness retinal necrosis despite systemic and intravitreal antifungal therapy. The authors noted that C. gattii can cause chorioretinitis similarly to C. neoformans, and that surgical debridement via vitrectomy is challenging. This is only the second detailed report of human C. gattii chorioretinitis in the ophthalmic literature.
Afkhamnejad et al. (2023) reported a case of primary orbital C. neoformans infection in a 20-year-old man who was initially considered immunocompetent 3). The orbital abscess extended intracranially through the frontal bone, requiring multidisciplinary management involving ophthalmology, neurosurgery, and infectious diseases. Immunological workup revealed low IgM levels, suggesting an undiagnosed humoral immune abnormality. To the authors’ knowledge, this was the first report of primary orbital cryptococcosis worldwide.
Anti-GM-CSF autoantibodies and disseminated cryptococcosis
Viola et al. (2021) conducted a literature review on the association between disseminated cryptococcosis and anti-GM-CSF autoantibodies, collecting 27 cases 6). All cases had CNS involvement, and 48% had concurrent pulmonary lesions. C. gattii was predominant (63%). Among 19 cases with known clinical outcomes, 13 (68%) achieved full recovery, while 6 (32%) had neurological or ophthalmic sequelae. The authors recommend testing for anti-GM-CSF autoantibodies in patients with disseminated cryptococcosis without known immunodeficiency.
Solís-Gómez R, Hernández-Dehesa IA, Adan-Ruiz A, Sánchez-Cruz AF, Argüelles-González E. Ophthalmoplegia as a Rare Initial Presentation of Cryptococcal Meningitis: A Case Report and Literature Review. Revista de la Facultad de Ciencias Medicas (Cordoba, Argentina). 2025;82(1):176-187. doi:10.31053/1853.0605.v82.n1.44952. PMID:40163835; PMCID:PMC12057709.
Willett KL, Dalvin LA, Pritt BS, Fida M, Kasten MJ, Olsen TW. Cryptococcus gattii endogenous chorioretinitis. American journal of ophthalmology case reports. 2022;25:101283. doi:10.1016/j.ajoc.2022.101283. PMID:35112022; PMCID:PMC8789595.
Afkhamnejad ER, Turner C, Reynoso D. A case of orbital cryptococcosis. American journal of ophthalmology case reports. 2023;30:101821. doi:10.1016/j.ajoc.2023.101821. PMID:36852304; PMCID:PMC9958422.
Petrakis V, Angelopoulou CG, Psatha E, et al. Recurrent Cryptococcal Meningitis in a Late Presenter of HIV: A Rare Case Report and Review of Literature. Am J Case Rep. 2023;24:e941714. doi:10.12659/ajcr.941714.
Tu A, Byard RW. Cryptococcosis and unexpected death. Forensic science, medicine, and pathology. 2021;17(4):742-745. doi:10.1007/s12024-021-00400-1. PMID:34324155; PMCID:PMC8320313.
Viola GM, Malek AE, Rosen LB, DiNardo AR, Nishiguchi T, Okhuysen PC, et al. Disseminated cryptococcosis and anti-granulocyte-macrophage colony-stimulating factor autoantibodies: An underappreciated association. Mycoses. 2021;64(6):576-582. doi:10.1111/myc.13247. PMID:33476401; PMCID:PMC11913175.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.