Leukemic Optic Neuropathy (LON) is an optic nerve dysfunction caused by direct infiltration of neoplastic leukocytes. The infiltration may involve the entire optic nerve or be limited to the optic sheath.
The optic nerve is a direct extension of the central nervous system (CNS), and LON in leukemia patients indicates CNS infiltration. LON is a neuro-oncologic emergency requiring immediate intervention to prevent permanent vision loss.
Even when systemic and bone marrow remission is presumed, the optic nerve can be a site of CNS relapse. The optic nerve is considered a “sanctuary site” for leukemic cells even if chemotherapy, imaging, and cerebrospinal fluid (CSF) tests are negative. This is because the blood-brain barrier (BBB) and blood-retinal barrier (BRB) impede drug penetration into the optic nerve, contributing to incomplete eradication of leukemic cells. Patients who have received prophylactic intrathecal chemotherapy still remain at risk for relapse and LON.
Epidemiology: Infiltration of the optic nerve occurs in up to 18% of acute leukemia and up to 16% of chronic leukemia. The incidence of CNS leukemia may be increasing due to improved survival rates from advances in chemotherapy and targeted therapy. Among representative causes of infiltrative optic neuropathy, leukemia is common in young to middle-aged adults, while malignant lymphoma and carcinomatous meningitis are more common in older adults. In pediatric acute leukemia, direct cellular infiltration of the optic nerve is considered frequent.
QCan leukemia affect the optic nerve even if the leukemia is in remission?
A
Even when the systemic and bone marrow are in remission, the optic nerve can be a site of CNS relapse. Because the optic nerve is a “sanctuary site” where drug penetration is hindered by the BBB and BRB, infiltration can occur even if chemotherapy, imaging, and CSF tests are all negative.
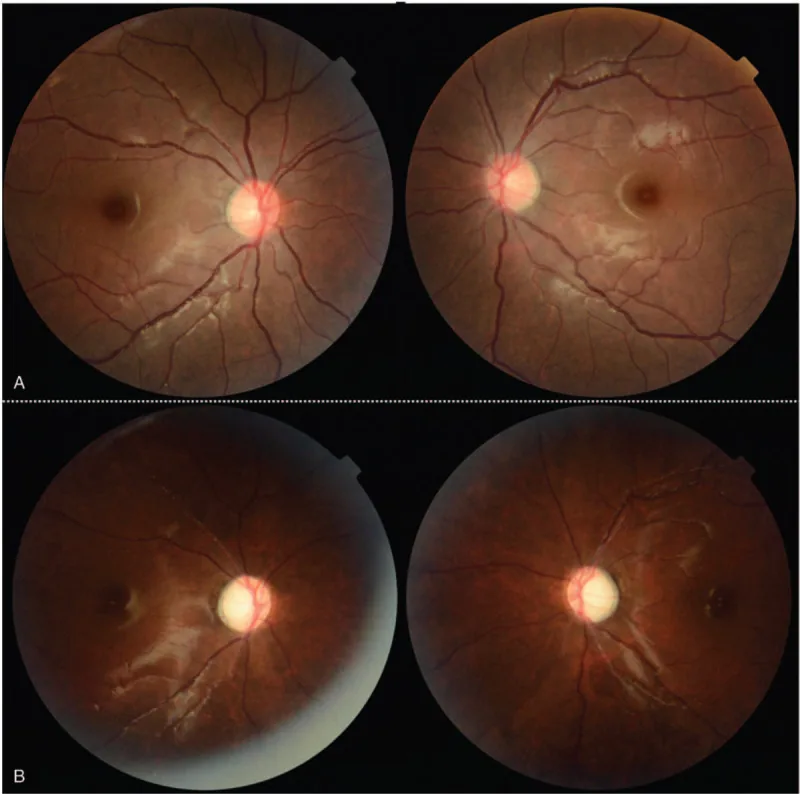
Woo Hyuk Lee, Sun Kyoung You, Yeon-Hee Lee. Bilateral optic neuropathy following vincristine chemotherapy: A case report with description of multimodal imaging findings. Medicine. 2021 Mar 5; 100(9):e24706. Figure 1. PMCID: PMC7939147. License: CC BY.
A complete neuro-ophthalmic examination is important. Best corrected visual acuity, RAPD, dilated fundus examination, anterior segment examination, intraocular pressure, and eye movements should be assessed. Visual field evaluation using automated perimetry and retinal nerve fiber layer (RNFL) evaluation using OCT are also performed.
Optic disc findings: Optic disc edema or pallor, and peripapillary cotton-wool spots may appear as optic nerve infiltration.
Position relative to the lamina cribrosa: Infiltration anterior to the lamina cribrosa may result in normal to mildly decreased visual acuity. Infiltration posterior to the lamina cribrosa presents with severe visual loss.
Form of retrobulbar optic neuropathy: When presenting as retrobulbar optic neuropathy, fundus findings may be normal in the early stage.
Mechanism of optic disc swelling: Three factors are involved: (1) papilledema due to increased intracranial pressure, (2) circulatory disturbance due to direct infiltration of leukemia cells, and (3) ischemic changes due to hemorrhagic diathesis and increased blood viscosity.
Unilateral or bilateral: Can occur in either eye; bilateral cases may present simultaneously.
OCT findings: RNFL thickening (due to infiltration) or thinning/disappearance.
Leukemic retinopathy may present with Roth spots and multilayered hemorrhages (preretinal, subretinal, intraretinal). These are secondary to underlying anemia and thrombocytopenia, not necessarily due to infiltration itself.
When perivascular infiltration occurs, retinal veins become dilated and tortuous (sausage-like changes), along with cotton-wool spots and vascular sheathing. Orbital infiltration or retrobulbar hemorrhage may cause eyelid edema, ptosis, proptosis, ocular motility disorders, and eye pain. Anterior segment infiltration may present with limbal infiltration, conjunctival thickening, edema, corkscrew vessels, pseudohypopyon, and secondary glaucoma.
QWhat fundus findings are observed in leukemic optic neuropathy?
A
The main optic nerve findings are optic disc edema or pallor, and peripapillary cotton-wool spots. Roth spots and multilayered hemorrhages (leukemic retinopathy) are also observed, but these are not necessarily due to infiltration and may be secondary to anemia or thrombocytopenia. Infiltration central to the lamina cribrosa presents with severe vision loss.
LON is caused by direct infiltration of leukemic cells. Infiltration occurs more frequently in acute types of leukemia.
The frequency by leukemia subtype in a review of 92 leukemia cases (including 35 LON cases) is shown [1].
Leukemia subtype
Classification
Acute lymphoblastic leukemia (ALL)
Most common
Chronic lymphocytic leukemia (CLL)
Second most common
Acute myeloid leukemia (AML)
Third most common
Chronic myeloid leukemia (CML)
Fourth most common
Among lymphomas, non-Hodgkin B-cell lymphoma (NHL) is most commonly associated [1]. Case reports and literature reviews of optic nerve infiltration in chronic lymphocytic leukemia have also been reported [4].
CNS infiltration occurs at initial presentation or at CNS relapse. Optic nerve infiltration may be present even when blood tests and imaging are normal during remission, making it difficult to exclude.
QWhich type of leukemia is more likely to cause optic neuropathy?
A
It occurs more commonly in acute leukemia. In a review of 92 cases, ALL was the most common, followed by CLL, AML, and CML. Among lymphomas, non-Hodgkin B-cell lymphoma is most frequently associated.
The diagnosis of LON is made through thorough and urgent ophthalmologic and oncologic evaluation. Emergency response is required when a leukemia patient presents with vision loss. Differential diagnoses include autoimmune, infectious, inflammatory, and drug-induced optic neuropathies, optic neuritis (idiopathic or demyelinating), ischemic optic neuropathy, and compressive optic neuropathy.
MRI and CT Scans
Brain and orbital MRI (with and without contrast): Contrast enhancement and thickening of the optic nerve may be observed. In some cases, it may be normal, and a negative result does not rule out LON. It is also useful for identifying lesions that can be biopsied.
CT/MRI: Can confirm enlargement of the retrobulbar optic nerve, but abnormalities may not be seen with infiltration limited to the optic disc.
Lumbar Puncture / Biopsy
Lumbar puncture (cytology + flow cytometry): Diagnosis is made by detecting leukemic blasts (>5/μL) in CSF. Results may be normal. FCM immunophenotyping can detect lymphoblasts with up to 100% sensitivity and specificity.
Optic nerve biopsy: Considered in cases of severe visual impairment when preliminary tests are inconclusive. The transorbital approach (transconjunctival) may be preferred over the intracranial approach.
Blood and Bone Marrow Tests
Complete blood count (CBC): In chronic leukemia, leukocytosis >100,000/μL. In acute leukemia, anemia, thrombocytopenia, leukopenia, or pancytopenia.
Peripheral blood smear: Search for blast cells and Auer rods.
Bone marrow biopsy: Definitive diagnosis of acute leukemia. Flow cytometry identifies the lineage of leukemic blasts.
Management of LON is multidisciplinary. Prompt consultation with an oncologist is recommended in all cases.
Orbital Radiation Therapy
Indications: Leukemia cells are radiosensitive, and this is positioned as a first-line treatment.
Regimen: A typical course is 2000 cGy delivered over 1–2 weeks. Significant improvement in vision is expected [3,5].
Prognostic Factors: The main factor determining treatment efficacy is the time from visual impairment to initiation of radiation therapy. Early initiation is crucial.
Intrathecal Chemotherapy
Characteristics: When used alone, efficacy may be limited. Massive infiltration of leukemia cells may act as a barrier between the optic nerve lesion and the CNS.
Limitations of chemotherapy: It is difficult to cross the blood-brain barrier and reach infiltrating cells in the optic nerve. Some reports question the effectiveness of intrathecal administration.
Combination therapy: The combination of intrathecal chemotherapy and orbital radiation is the mainstay of treatment.
Corticosteroids may be used as an adjunct. However, they can alter CSF diagnostic results, pathological findings, and neuroimaging findings, so it is recommended to establish the diagnosis before starting treatment.
QIs intrathecal chemotherapy alone insufficient?
A
Intrathecal chemotherapy alone may have limited efficacy. Massive infiltration of leukemia cells can act as a barrier between the optic nerve lesion and the CNS, and combination with orbital radiation is the mainstay of treatment.
CNS infiltration occurs as part of initial symptoms or as a sign of leukemia relapse.
The pathways of spread to the optic nerve are as follows:
Spread from the pia mater: Spreads from the pia mater to the optic nerve via the pial septae and perivascular spaces.
Spread to the perineurium and endoneurium: Expands from the perineurium and endoneurium to the brain surface and cranial nerves.
Perivascular accumulation: Leukemia cells accumulate around blood vessels within the optic nerve, impairing blood flow.
Axonal transport stasis: Infiltration of the pial septa causes axoplasmic flow stasis. This results in delayed axonal conduction and ultimately leads to demyelination.
The following three mechanisms are involved in the pathogenesis of papilledema:
Choked disc: Associated with increased intracranial pressure.
Circulatory disturbance: Blood flow obstruction due to direct infiltration of leukemia cells.
Ischemic changes: Vascular occlusion due to hemorrhagic diathesis and increased blood viscosity.
Leukemic cell infiltration around retinal blood vessels leads to vascular occlusion, causing venous dilation, tortuosity, cotton wool spots, and sheathing. The blood-brain barrier (BBB) and blood-retinal barrier (BRB) prevent therapeutic drugs from penetrating the optic nerve, which is a fundamental cause of incomplete eradication of leukemic cells.
Myers KA, Nikolic A, Romanchuk K, et al. Optic neuropathy in the context of leukemia or lymphoma: diagnostic approach to a neuro-oncologic emergency. Neurooncol Pract. 2017;4(1):60-66. PMID: 31386008.
Johnson GM, Rossen JL, Simon SS, et al. Leukemic Optic Neuropathy in Pediatric Patients: A Case Series. J Pediatr Ophthalmol Strabismus. 2024;61(1):67-72. PMID: 37227013.
Lee V, Farooq AV, Shah HA. Leukemic and Lymphomatous Optic Neuropathy: A Case Series. J Neuroophthalmol. 2021;41(4):e796-e802. PMID: 34629409.
Liu L, Hadyah S, Park A, et al. Leukemic infiltration of the optic nerve in chronic lymphocytic leukemia: A case report and review of literature. Leuk Res Rep. 2023;20:100391. PMID: 37711672.
Verter E, Yang A, Lim RP. Leukemic Optic Nerve Infiltration Responds to Radiation and Blinatumomab. Ophthalmology. 2018;125(5):746. PMID: 29681296.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.