Xerophthalmia is a general term for a series of eye diseases caused by severe vitamin A deficiency (VAD). Vitamin A is a fat-soluble vitamin essential for normal differentiation of the corneal and conjunctival epithelium, and its deficiency leads to progressive damage to the conjunctiva, cornea, and retina.
According to WHO estimates, approximately 228 million children worldwide suffer from VAD, and 250,000 to 500,000 children become blind each year due to xerophthalmia 3). In developed countries, it is rare; the prevalence in the United States is 0.3% (2013 CDC survey) 1).
However, the prevalence of VAD is higher in patients with certain underlying diseases 1).
Children with inflammatory bowel disease (IBD): 16% (more common in Crohn’s disease than ulcerative colitis)
In Japan, vitamin A deficiency is almost never seen, but it is known to rarely occur in association with eating disorders or alcohol dependence.
QCan xerophthalmia occur in Japan?
A
In Japan, VAD due to malnutrition is extremely rare, but it can occur in association with eating disorders, intestinal malabsorption due to alcohol dependence, or impaired absorption of fat-soluble vitamins after gastrectomy. In recent years, reports have also been seen of extreme picky eating in autism spectrum disorder as a cause.
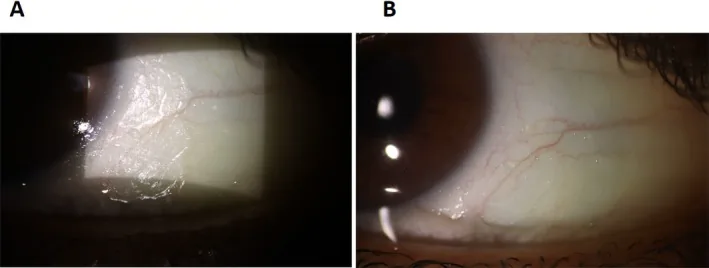
Shoeibi N, et al. Xerophthalmia and Nyctalopia as Presenting Signs of Vitamin A Deficiency in a Patient With Rapid Intentional Weight Loss: A Case Report and Literature Review. Clinical Case Reports. 2025;13(9):e70896. Figure 1. PMCID: PMC12441006. License: CC BY.
Both A and B show foamy, white Bitot’s spots on the bulbar conjunctival surface. They indicate dry corneal and conjunctival surface changes seen in vitamin A deficiency.
Night blindness: The earliest symptom. Perceived as decreased vision in dark places.
Ocular irritation symptoms: Dry eye sensation, foreign body sensation, photophobia
Decreased visual acuity: Worsens with progression of corneal opacity
Eye pain: Occurs when accompanied by corneal ulcer
In children, corneal ulcers may suddenly develop after measles or diarrhea without initial signs of VAD. Behavioral changes such as becoming passive or fearful in dark places can be signs of VAD.
Clinical findings (findings confirmed by physician examination)
The WHO classifies xerophthalmia into the following stages (1982).
WHO classification
Pathology
Risk of blindness
XN
Night blindness
None
X1A / X1B
Conjunctival xerosis / Bitot’s spots
None
X2
Corneal xerosis
Present
X3A / X3B
Corneal ulcer / Keratomalacia
High
XS / XF
Corneal scarring / Fundus changes
Depends on scarring
Early stage (XN to X1B)
Night blindness (XN): Due to impaired rhodopsin formation in rod cells. Begins to appear when serum retinol is below 1.0 μmol/L3).
Conjunctival xerosis (X1A): Loss of conjunctival luster and dryness. Caused by goblet cell loss and decreased mucin secretion.
Bitot spots (X1B): Mixed deposits of keratinized epithelial cells and Corynebacterium xerosis. Appear as triangular, foamy white deposits on the temporal bulbar conjunctiva.
Advanced to severe stage (X2 to X3B)
Corneal xerosis (X2): The cornea loses its luster and becomes cloudy. Presents as punctate keratopathy and can rapidly progress to corneal ulcer.
Keratomalacia (X3A/B): Melting of the corneal stroma due to liquefactive necrosis. The most severe form, which can lead to corneal perforation within days.
Corneal scarring (XS): Scarring after corneal ulcer. Often symmetric and bilateral.
Advanced cases result in irreversible complications. In a report of three children with autism, severe VAD (serum vitamin A ≤0.12 μmol/L) led to corneal perforation requiring enucleation, or permanent visual impairment (best vision hand motion to 0.01) due to optic atrophy2).
Khan et al. (2021) confirmed squamous metaplasia and keratin pearl formation in a conjunctival biopsy of a 24-year-old woman after intestinal resection5). This finding provides histological evidence of ocular surface changes due to VAD.
QDo Bitot spots disappear with treatment?
A
Bitot spots improve within about two weeks of vitamin A supplementation1). However, recovery from night blindness may take four weeks or longer. If treatment is started by the stage of corneal xerosis, complete visual recovery can be expected, but progression to keratomalacia may leave scarring.
In developing countries, chronic malnutrition is the leading cause. In developed countries, the following issues are problematic:
Extreme picky eating: Common in children with autism spectrum disorder. It occurs when only limited foods such as noodles or french fries are consumed 2)3)
Chronic alcoholism: Leads to depletion of liver stores and intestinal malabsorption simultaneously
Zinc deficiency: Suppresses hepatic synthesis of retinol-binding protein (RBP), impairing vitamin A transport 1)
Measles: Reduces serum retinol by more than 30%. The mechanism is thought to be suppression of RBP synthesis 1)
Children with coexisting night blindness and Bitot spots have a mortality rate nine times higher than children with subclinical VAD3)
QIs there a risk of vitamin A deficiency in children with picky eating?
A
Extreme picky eating (consuming only specific foods) associated with autism spectrum disorder or Down syndrome is an important risk factor for VAD2)3). Regular monitoring of serum vitamin A levels is recommended in children with picky eating.
Slit-lamp microscopy under dilated pupils is fundamental. Assess loss of conjunctival luster, Bitot spots, and corneal opacity. It is important to obtain a dietary history, history of malabsorption, and alcohol consumption history.
Serum vitamin A (retinol): Reference range 20–60 mcg/dL. Ocular symptoms appear at levels below 10 mcg/dL. However, because blood levels are maintained by liver stores, a normal value does not rule out VAD.
Serum retinol-binding protein (RBP): Reference range 30–75 μg/mL
Serum zinc: Reference range 75–120 mcg/dL. Check for concurrent zinc deficiency.
WHO recommends high-dose oral vitamin A for xerophthalmia (including cases with severe malnutrition or measles) 1).
Age group
Single dose (IU)
0–5 months
50,000
6–11 months
100,000
12 months and older
200,000
The dosing schedule is three doses: on day 1, day 2, and day 14 1). Intramuscular injection is recommended in cases of malabsorption 1)4). If zinc deficiency is present, concurrent zinc supplementation is necessary.
Lubrication of the ocular surface with artificial tears and hyaluronic acid eye drops is performed. In cases of corneal perforation, full-thickness corneal transplantation may be indicated. In complex cases with limbal stem cell deficiency such as aniridia, high-dose vitamin A (200,000 IU) is administered along with antiglaucoma medications and topical antibiotics 6).
Sharma et al. (2021) reported a 12-year-old girl after Frey surgery whose keratoconjunctival findings completely resolved within two weeks of intramuscular and oral vitamin A administration, with visual acuity recovering to 20/20 4). Serum retinol normalized at 12 weeks.
Bitot spots improve about 2 weeks after starting treatment, but recovery from night blindness takes at least 4 weeks 1). When keratomalacia occurs, recovery is difficult, and scarring or permanent visual impairment remains. About two-thirds of children who develop keratomalacia die within a few months.
QHow soon will improvement occur after starting treatment?
A
If the condition is up to xerosis of the cornea (X2), vitamin A supplementation can improve ocular findings within 2 weeks, and full recovery of vision can be expected 4). Bitot spots also improve in about 2 weeks, but night blindness may take 4 weeks or more 1). If keratomalacia has developed, irreversible scarring may remain.
Vitamin A is a collective term for retinol, retinal, retinoic acid, etc., and is ingested as preformed vitamin A (from animal foods) or provitamin A carotenoids (from green and yellow vegetables). After absorption in the duodenum, 80–90% of the total body amount is stored in hepatic stellate cells. It is released into the blood bound to prealbumin (transthyretin) and retinol-binding protein (RBP).
The main functions of vitamin A in the eye are the following two.
Maintenance of ocular surface epithelium: Controls normal differentiation of conjunctival and corneal epithelium. Vitamin A stimulates the synthesis of mucin 4 (MUC4) and promotes mucin secretion from conjunctival epithelium 7)
Visual cycle of the retina: Retinol is an essential cofactor for rhodopsin formation in rod cells. VAD impairs rod function, leading to night blindness
When VAD occurs, overexpression of keratinocyte transglutaminase in the corneal and conjunctival epithelium leads to abnormal keratinization 7). In this process, goblet cells disappear and mucin secretion decreases.
The pathology progresses stepwise in the following order.
Rod cell dysfunction: Impaired rhodopsin formation → night blindness (XN)
In the stage of keratomalacia, increased collagenase activity causes rapid melting of the corneal stroma, which can lead to perforation within just a few days.
7. Latest Research and Future Perspectives (Investigational Reports)
According to the TFOS DEWS III report, oral vitamin A supplementation improved tear quality in dry eye patients but did not affect tear volume 8). Topical vitamin A eye drops have shown more stable tear film stability and ocular surface improvement, and combination therapy with cyclosporine A is also being investigated 8).
Azmi et al. (2023) reported severe ocular xerosis due to VAD in three children with autism, emphasizing the existence of irreversible cases leading to optic atrophy2). The importance of regular serum vitamin A level screening in children at high risk of picky eating, such as those with autism spectrum disorder or Down syndrome, has been advocated.
After bariatric surgery such as Roux-en-Y gastric bypass, the risk of VAD is high, and the need for monitoring ocular surface changes postoperatively has been pointed out 7). A report found VAD in 35% of patients at 6 weeks post-surgery, highlighting the need for early detection and intervention systems.
Khan Z, Cox V, Creagmile J, Oboh-Weilke A. Nyctalopia and Xerophthalmia in a Patient With Crohn’s Induced Vitamin A Deficiency. Cureus. 2023;15(8):e42961.
Azmi AZ, Patrick S, Isa MIB, Ab Ghani S. A Multifaceted Presentation of Xerophthalmia in Autistic Patients. Cureus. 2023;15(11):e49172. doi:10.7759/cureus.49172. PMID:38130530; PMCID:PMC10734353.
Ifwat A, Liew OH, Abdul Hamid H, Patrick S, Ab Ghani S. Xerophthalmia in Picky Eater Children. Cureus. 2022;14(3):e22846. doi:10.7759/cureus.22846. PMID:35399490; PMCID:PMC8980242.
Sharma S, Murthy SI, Bhate M, Rathi V. Xerophthalmia due to vitamin A deficiency following Frey’s procedure for chronic calcific pancreatitis. BMJ case reports. 2021;14(5). doi:10.1136/bcr-2021-242710. PMID:34031093; PMCID:PMC8149307.
Khan SI, Kumar A, Panda PK, Gupta N. Xerophthalmia with secondary malabsorption syndrome in a young lady. Journal of family medicine and primary care. 2021;10(9):3515-3518. doi:10.4103/jfmpc.jfmpc_1020_21. PMID:34760784; PMCID:PMC8565163.
Magdum R, Rao RK, Ganesh A, Chaudhary N, Vatkar V. Unravelling the Enigma of Ocular Complexity: Delving into Aniridia, Xerophthalmia, Corneal Ulcer, Keratomalacia, and Beyond. Cureus. 2024;16(7):e64631. doi:10.7759/cureus.64631. PMID:39149643; PMCID:PMC11325210.
Markoulli M, Ahmad S, Arcot J, Arita R, Benitez-Del-Castillo J, Caffery B, et al. TFOS Lifestyle: Impact of nutrition on the ocular surface. The ocular surface. 2023;29:226-271. doi:10.1016/j.jtos.2023.04.003. PMID:37100346.
Stapleton F, Abad JC, Engel L, Gomes JAP, Nichols KK, Schaumberg DA, et al. TFOS DEWS III Management and Therapy Report. Am J Ophthalmol. 2025;262:1-55.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.