Wessely immune ring is a sterile ring-shaped infiltration in the corneal stroma resulting from an immune response to foreign antigens. In 1911, Wessely recorded a reproducible immune reaction in rabbit corneas exposed to bovine or equine serum proteins, first reporting it as the “Wessely phenomenon.”
In 1956, Morawiecki proposed the role of immune complex-mediated complement activation. Later, it was found that other antigens, such as bacterial endotoxins, can also trigger antibody-independent properdin-mediated alternative complement pathway activation.
It may appear during the course of infectious keratitis or as a non-infectious corneal reaction.
QIn what situations is Wessely immune ring seen?
A
Wessely immune ring appears in various situations. In infectious cases, it is associated with keratitis caused by Pseudomonas, Acanthamoeba, herpes, fungi, etc. In non-infectious cases, it has been reported with chronic contact lens use, after excimer laser treatment, eye drops (e.g., diclofenac), corneal chemical trauma, Behçet’s disease, and recurrent corneal erosion. In all cases, the essence is an immune reaction in the corneal stroma to foreign antigens.
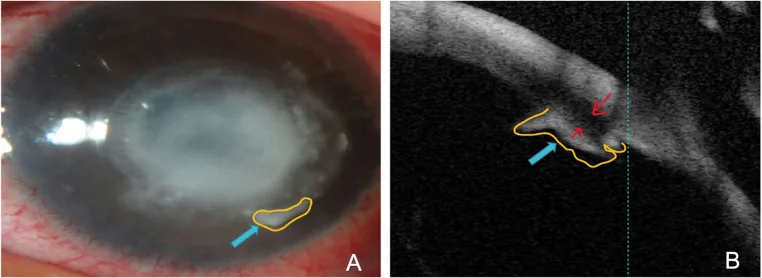
Alreshidi SO, et al. Differentiation of acanthamoeba keratitis from other non-acanthamoeba keratitis: Risk factors and clinical features. PLOS ONE. 2024;19(3):e0299492. Figure 4. PMCID: PMC10931457. License: CC BY.
A is a slit-lamp photograph showing a ring-shaped corneal opacity, and B is an anterior segment OCT of the same area. It can help confirm the location and depth of the immune ring formed around the corneal infiltrate.
The subjective symptoms of Wessely immune ring are related to the underlying disease. The immune ring itself usually does not significantly affect vision.
Eye pain: Present when associated with infectious keratitis.
Foreign body sensation and burning sensation: Appear depending on the degree of corneal epithelial damage.
Blurred vision: Occurs when corneal stromal opacity extends to the pupillary area.
Photophobia and conjunctival injection: Present depending on the degree of inflammation.
Tearing and purulent discharge: Become prominent when complicated by infectious keratitis.
Clinical Findings (Findings Confirmed by Physician Examination)
A typical Wessely immune ring is a ring-shaped infiltrate within the corneal stroma, formed near the limbus. It appears as a visible ring separated from the central infectious focus by a clear zone.
Herpetic immune stromal keratitis: Appears as a deep opacity ring in the mid-stroma. Usually located centrally or paracentrally, and may appear to surround an area of disciform corneal endotheliitis.
Acanthamoeba keratitis: Corneal stromal ring infiltrate appears in about 15% of patients1). Ring infiltrate is defined as one of the “severe inflammatory complications (SIC)“1).
Similarity to pseudogerontoxon: In catarrhal corneal ulcer, an infiltrate parallel to the limbus is observed, with a 1–2 mm clear zone between the limbus and the infiltrative lesion. It is a sterile infiltrate due to type III allergic reaction (complement activation + neutrophil infiltration), showing a pathophysiology similar to Wessely immune ring.
Gram-negative bacilli: Pseudomonas aeruginosa is a typical example. Endotoxin activates the alternative pathway, leading to early appearance of immune rings.
Herpesviruses: Seen in immune stromal keratitis caused by herpes simplex virus (HSV) and varicella-zoster virus (VZV).
Acanthamoeba: Because the clinical course is prolonged, the appearance of immune rings is also delayed.
Fungi: Reported in fungal keratitis and Pythium insidiosum keratitis.
Contact lenses: Thought to be an immune reaction to bacterial antigens (especially endotoxins of gram-negative bacilli) associated with chronic use. Contamination of storage solutions can also be a cause.
Excimer laser: Reported after PRK and PTK. Cross-reactivity between heat shock proteins and circulating antibodies to bacterial HSP has been proposed as a hypothesis.
In Acanthamoeba keratitis, ring infiltrates and scleritis are defined as “severe inflammatory complications (SIC)” 1). The following independent risk factors for SIC have been identified 1).
Wessely immune ring is diagnosed based on clinical findings using a slit-lamp microscope. When ring-shaped infiltration in the corneal stroma is observed, differentiation from infectious ring infiltration is most important.
Ring infiltrates are also commonly seen in fungal keratitis and Acanthamoeba keratitis2). HSV, varicella-zoster virus, and EB virus can also cause immunologically mediated corneal infiltrates that may resemble bacterial, fungal, or Acanthamoeba keratitis2).
Necrosis: Accompanied by necrotic findings in the corneal stroma.
Anterior chamber reaction: Anterior chamber inflammation including hypopyon.
On the other hand, mild infiltrates outside the ulcer border that respond to steroid eye drops suggest a “pure” Wessely immune ring area.
QHow to differentiate between infectious and sterile ring infiltrates?
A
Infectious ring infiltrates show marked inflammatory findings such as pain, severe conjunctival hyperemia, epithelial defect, purulent discharge, necrosis, and anterior chamber reaction. Sterile Wessely immune rings appear at a distance from the central infectious focus across a clear zone, with mild inflammation and response to steroid eye drops. However, since both can form simultaneously during microbial keratitis, when ring infiltrates are observed, infection should be suspected first and culture tests performed as a rule.
Usually no specific treatment is required. Clinically, steroid eye drops may be administered. If it is a “truly sterile” infiltrate, it usually heals quickly and completely.
This is a sterile infiltrate occurring in the peripheral cornea due to a type III allergic reaction (complement activation + neutrophil infiltration) to staphylococcal antigens, showing a similar condition to Wessely immune ring. Combination of antibiotics and low-concentration steroid eye drops is effective, and for long-term management, eyelid margin cleaning and antibiotic eye ointment application are important.
The core of Wessely immune ring pathology is the interaction between foreign antigens and antibodies diffusing into the stroma from the limbal vasculature.
Exogenous antigens (microbial antigens, endotoxins, etc.) are present in the corneal stroma.
IgG antibodies diffusing from limbal vessels bind to antigens, forming immune complexes.
Immune complexes activate the complement system.
Chemotactic factors (C3a, C5a) are produced, recruiting polymorphonuclear leukocytes (mainly neutrophils) into the stroma.
Accumulation of neutrophils forms a ring-shaped infiltrate around the corneal limbus.
Classical pathway: Antigen-antibody complexes bind to C1q and activate it. The immune ring appears 10–14 days after infection onset.
Alternative pathway (properdin pathway): Endotoxins, etc., directly activate C3 independently of antibodies. In Pseudomonas aeruginosa keratitis or with pre-sensitized antigens, the immune ring appears early, within 1–5 days.
Involvement of both pathways may explain the variability in the time from symptom onset to appearance of the immune ring.
The reason the immune ring forms in a ring shape around the limbus is that antibodies diffuse from limbal vessels toward the corneal center, and the site where they bind in an optimal ratio (equivalence zone) with antigens in the corneal stroma occurs at a certain distance from the limbus. This reaction follows a mechanism similar to the Arthus reaction (local type III allergic reaction).
QWhy does the infiltrate form a ring?
A
Antibodies diffuse radially from limbal vessels toward the corneal center. Meanwhile, antigens diffuse from the central infection site or foreign material toward the periphery. The site where both bind in an optimal ratio (equivalence zone) becomes a ring-shaped zone at a certain distance from the limbus, where immune complexes deposit intensively. Complement activation and neutrophil recruitment also concentrate at this site, resulting in a ring-shaped infiltrate.
In a retrospective analysis of the Acanthamoeba keratitis cohort (culture- or pathology-confirmed cases) at Moorfields Eye Hospital from 1991 to 2012, ring infiltrate and scleritis were defined as “severe inflammatory complications (SIC)” 1). Independent risk factors for SIC were age >34 years (OR 2.36) and steroid use before AAT (OR 2.56) 1).
Stratified analysis showed that in patients without scleritis, ring infiltrate was a strong independent factor for poor prognosis (OR 5.57; 95% CI 2.02–15.39; P=0.001) 1). In contrast, when scleritis was present, the risk of poor prognosis was high regardless of the presence of ring infiltrate, and the additional impact of ring infiltrate was small 1). These results suggest that scleritis and ring infiltrate are related but may have different pathophysiology 1).
Wessely immune rings have been reported after PRK and PTK. Previously, this was thought to be caused by the release of denatured DNA proteins at the edge of the laser ablation zone, but a recent hypothesis proposes that mammalian heat shock proteins (HSPs) produced after physical stress cross-react with circulating antibodies against bacterial HSPs derived from past infections.
This is a rare ocular surface disease reported in association with handling palytoxin (PTX)-producing corals. PTX acts on the Na-K ATPase pump, potentially causing corneal epithelial detachment, Wessely immune ring formation, and peripheral corneal thinning. Severity ranges from mild ocular surface damage to corneal melting and perforation.
Carnt N, Robaei D, Watson SL, et al. Demographic and clinical risk factors associated with Acanthamoeba keratitis in a large UK case series of 221 patients. Br J Ophthalmol. 2018;102(10):1431-1435.
American Academy of Ophthalmology Cornea/External Disease Preferred Practice Pattern Panel. Bacterial Keratitis Preferred Practice Pattern. Ophthalmology. 2024;131(2):P1-P47.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.