HLA-B27-associated acute anterior uveitis (HLA-B27-AAU) is an acute, recurrent, non-granulomatous anterior uveitis that occurs predominantly in individuals positive for human leukocyte antigen B27 (HLA-B27). Acute anterior uveitis is an inflammation of the anterior segment of the eye that develops acutely, often accompanied by severe eye pain in addition to visual impairment. It frequently occurs in association with various systemic diseases and is often HLA-B27 positive. In such cases, it is called HLA-B27-positive-associated uveitis, and it is often complicated by other HLA-B27-associated diseases such as ankylosing spondylitis, Reiter’s syndrome, psoriatic arthritis, and inflammatory bowel disease.
Approximately 50% of all acute anterior uveitis cases are associated with HLA-B27, making it the most common identifiable cause of non-infectious uveitis worldwide 2). In a 2009 prospective study, acute anterior uveitis accounted for 6.6% (250/3,060 cases) of all uveitis, and HLA-B27-associated uveitis accounted for 1.5% (46/3,060 cases) 1).
Ethnic distribution of HLA-B27:
Ethnicity/Region
HLA-B27 positivity rate
Papua New Guinea, Pawaiya tribe
53%
Canada, Haida tribe
50%
Northern Scandinavia
14–16%
Caucasians
8–10%
Non-Hispanic White (USA)
7.5%
African American
2–4%
The HLA-B gene locus encodes MHC class I surface antigens that present antigens to CD8+ T cells, with over 105 subtypes and 132 gene alleles. The amino acid composition of the antigen-binding groove of HLA-B27 is unique, suggesting involvement in autoimmune responses.
In Japan, the frequency of HLA-B27-associated AAU is considered lower than in Western countries. The HLA-B27 positivity rate and its proportion among all uveitis cases vary greatly depending on the target population and diagnostic system 1, 2). The interval between attacks ranges from several months to several years 1). Genetic analysis studies have reported both genetic similarities and differences between AAU and ankylosing spondylitis 3).
QDoes being HLA-B27 positive always lead to uveitis?
A
The majority of HLA-B27-positive individuals do not develop uveitis. HLA-B27 is a genetic factor that increases disease susceptibility, but other environmental and immune factors are also involved in the onset. Some cases of uveitis occur without any systemic disease.
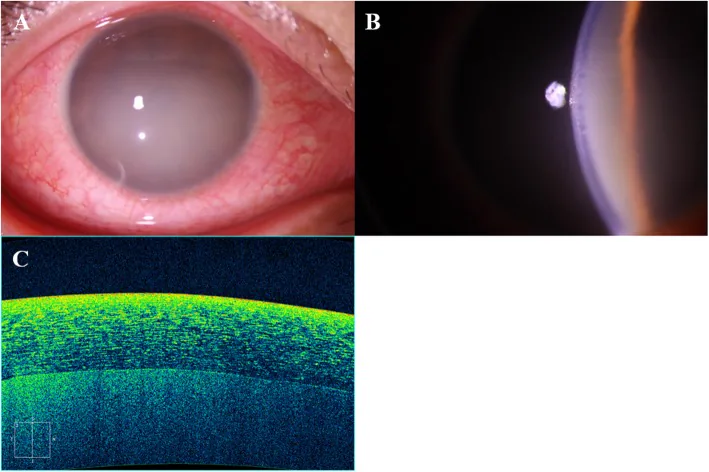
Kim JI, et al. A case of severe flare reaction observed in HLA B27 associated acute anterior uveitis. BMC Ophthalmol. 2020. Figure 1. PMCID: PMC7247201. License: CC BY.
The right eye shows intense conjunctival injection and milky-white opacity in the anterior chamber, obscuring iris details. Slit-lamp examination and anterior segment OCT confirm severe anterior chamber flare, representing typical inflammatory findings of acute anterior uveitis.
Redness: Severe conjunctival and ciliary injection is observed.
Decreased visual acuity: Occurs due to anterior chamber opacity and corneal changes.
Floaters: May be reported when accompanied by mild vitreous opacity.
Inflammatory episodes usually resolve within 2 months and recur on average 1–2 times per year. They often occur alternately in the right and left eyes, and simultaneous bilateral onset is extremely rare.
Anterior chamber inflammatory cells and flare: Numerous inflammatory cells and fibrin fill the anterior chamber.
Hypopyon: Predominantly composed of fibrin, highly viscous, and often irregularly shaped with a slightly elevated center1). May be accompanied by angle hypopyon1).
Anterior chamber fibrin: Adheres to the iris or anterior lens surface, temporarily covering the pupillary area, leading to decreased visual acuity.
Keratatic precipitates (KP) and corneal edema: Fine non-granulomatous KP, Descemet’s membrane folds, and corneal edema1).
Iris and angle findings
Posterior synechiae: Frequently formed. Visual recovery may be delayed for several weeks after inflammation subsides due to residual anterior vitreous opacity1).
Iris bombé: When posterior synechiae involve the entire circumference, aqueous humor flow is blocked, causing acute angle-closure glaucoma.
Low intraocular pressure: In acute inflammation, intraocular pressure often decreases due to reduced ciliary body function.
Systemic symptoms include low back pain (inflammatory back pain: worsens at rest, improves with exercise), inflammatory bowel disease symptoms, and psoriatic rash. In ankylosing spondylitis, bamboo spine may be seen on X-ray 1).
QWhy is intraocular pressure often low in uveitis?
A
In acute inflammation, ciliary body function is impaired, reducing the production of intraocular fluid (aqueous humor), which tends to lower intraocular pressure. On the other hand, obstruction of the trabecular meshwork by inflammatory cells or products, or iris bombé due to posterior synechiae, can increase intraocular pressure.
HLA-B27-associated AAU is a non-infectious anterior uveitis caused by immunological mechanisms. HLA-B27-associated diseases are classified as seronegative spondyloarthropathies (SpA). These include ankylosing spondylitis, reactive arthritis (formerly Reiter’s disease), psoriatic arthritis, and IBD-associated arthritis. The HLA-B27 positivity rate is over 90% in AS and about 70% in reactive arthritis.
Ankylosing spondylitis (AS): Most common complication. 19.2–50% of patients with this disease have the complication. Acute anterior uveitis develops in 25–30% of AS patients. Onset occurs in the teens to twenties, with a male-to-female ratio of 5:1 to 15:1. HLA-B27 is positive in over 90%.
Psoriasis: Complication with skin disease.
Inflammatory bowel disease (IBD): Association with ulcerative colitis and Crohn’s disease (gut-joint-eye axis).
Reactive arthritis (formerly Reiter’s disease): Association with arthritis occurring after infection. HLA-B27 positive in about 70% of cases.
Even in HLA-B27-negative cases, the clinical presentation of acute anterior uveitis may be difficult to clearly distinguish from B27-positive cases2).
Onset tendency: Age of onset is most commonly between 20 and 40 years. Men are 1.5 to 2.5 times more likely to develop it than women. Onset is more frequent in men and younger individuals1).
Interdepartmental collaboration when SpA is present1)
If SpA is suspected, collaboration with the following specialists is important alongside ophthalmological treatment.
Orthopedics: High rate of ankylosing spondylitis. Confirmation of bamboo spine and joint treatment.
Gastroenterology: Association with ulcerative colitis and Crohn’s disease.
Collagen disease/internal medicine: Management of reactive arthritis and introduction of immunosuppressants/biologics
Dermatology: Complication of psoriasis
QIs it necessary to check for spondyloarthritis?
A
The complication rate of SpA (spondyloarthritis) is high, ranging from 19.2% to 50%. Inflammatory back pain (low back pain that worsens at rest and improves with exercise) particularly requires further examination. Co-management with orthopedics, gastroenterology, rheumatology, and dermatology is important, and early diagnosis and treatment of SpA may help prevent recurrence of ocular inflammation.
There are no clear diagnostic criteria 1). Diagnosis is based on a comprehensive assessment of acute unilateral non-granulomatous anterior uveitis, HLA-B27 positivity, and presence of SpA. Iritis in HLA-B27-positive and -negative patients cannot be distinguished by clinical symptoms alone, but HLA-B27-positive patients are more often male and have younger onset. HLA testing is not mandatory due to cost, but it is important to check for a history of ankylosing spondylitis, inflammatory bowel disease, and psoriasis, as well as systemic symptoms.
Tests:
HLA class I test: HLA-B27 typing1)
Sacroiliac joint X-ray: To confirm ankylosing spondylitis. Check for bamboo spine1)
Fluorescein fundus angiography: May show hyperfluorescence of the optic disc1)
Syphilis serology, ACE, lysozyme: To rule out infection and sarcoidosis
Cyclosporine: The only immunosuppressive agent approved for uveitis under health insurance in Japan1). Indications: non-infectious uveitis resistant to systemic steroids, difficult to taper, or with intolerable side effects
Azathioprine and methotrexate are not covered by health insurance1)
Biologics (TNF inhibitors):1)
Infliximab: 5 mg/kg intravenous infusion. Administered at weeks 0, 2, and 6, then every 8 weeks. Approved for Behçet’s disease refractory retinal uveitis.
Adalimumab: Initial dose 80 mg subcutaneously, then 40 mg at week 1, followed by 40 mg every 2 weeks. Approved for non-infectious intermediate, posterior, or panuveitis.
Not approved for anterior uveitis alone: Use in isolated HLA-B27 acute anterior uveitis is not indicated. In cases with spondyloarthritis, TNF inhibitors may be introduced for SpA treatment, which can reduce the frequency of ocular inflammation recurrence.
Contraindications: Active tuberculosis, infections, congestive heart failure, malignancy, demyelinating diseases1).
Administer in collaboration with a rheumatology department1).
QWill uveitis recur immediately after stopping treatment?
A
HLA-B27-associated acute anterior uveitis is recurrent, but it does not always recur after stopping treatment. On average, relapses occur 1–2 times per year, but the frequency varies greatly among individuals. When systemic disease (SpA) is present, its treatment (e.g., biologics) may also help suppress ocular recurrences 1).
HLA-B27, as an MHC class I molecule, forms a trimer (MHC heavy chain, β2-microglobulin, and peptide) and presents antigens to CD8+ T cells. The antigen-binding groove of HLA-B27 has a unique amino acid composition, and several mechanisms such as molecular mimicry and misfolding hypotheses have been proposed, but the process is not fully understood.
In HLA-B27-associated diseases (correlation with AS, IBD, psoriasis, and Reiter’s disease), HLA-B27 is positive in over 90% of AS cases and about 70% of reactive arthritis cases. AAU and AS share genetic similarities and differences 3).
The concept of the gut-joint-eye axis, in which IBD (gastrointestinal inflammation) affects joint and eye inflammation, has been proposed, and alterations in the gut microbiota may contribute to the development of spondyloarthritis and uveitis.
Pathology of hypopyon: predominantly neutrophils, viscous and elevated shape — reflecting a different pathology from the thin, watery neutrophil-rich hypopyon in Behçet’s disease.
The clinical course of acute onset, short-term resolution, and recurrence reflects the characteristics of a self-limited immune response. Visual prognosis is generally good with appropriate treatment, but the duration of inflammation is usually 1 to 2 months, often taking longer to heal compared to iritis in Behçet’s disease.
7. Latest Research and Future Perspectives (Investigational Reports)
In HLA-B27-associated acute anterior uveitis, a rare complication of persistent pupillary dilation after an acute inflammatory episode has been reported. Alkhaldi et al. (2025) reported a case of a 38-year-old woman with HLA-B27-associated recurrent anterior uveitis who developed bilateral irreversible mydriasis (6 mm fixed) 4). A mechanism has been proposed in which ischemia of the iris sphincter occurs when three factors—anterior uveitis, elevated intraocular pressure, and use of mydriatic agents—overlap.
Reports are increasing that adalimumab and infliximab reduce the frequency of recurrence in patients with SpA-associated AAU. However, their indication for AAU alone remains investigational internationally. The impact of IL-17 inhibitors (e.g., secukinumab) indicated for AS on AAU recurrence is a topic for future study 1).
Robinson PC, Claushuis TA, Cortes A, Martin TM, Evans DM, Leo P, Mukhopadhyay P, Bradbury LA, Cremin K, Harris J, Maksymowych WP, Inman RD, Rahman P, Haroon N, Gensler L, Powell JE, van der Horst-Bruinsma IE, Hewitt AW, Craig JE, Lim LL, Wakefield D, McCluskey P, Voigt V, Fleming P, Spondyloarthritis Research Consortium of Canada, Australio-Anglo-American Spondylitis Consortium, International Genetics of Ankylosing Spondylitis Consortium, Wellcome Trust Case Control Study 2, Mariapia Degli-Esposti, Degli-Esposti M, Pointon JJ, Weisman MH, Wordsworth BP, Reveille JD, Rosenbaum JT, Brown MA.. Genetic dissection of acute anterior uveitis reveals similarities and differences in associations observed with ankylosing spondylitis. Arthritis Rheumatol. 2015;67(1):140-151. doi:10.1002/art.38873. PMID:25200001; PMCID:PMC4302162.
Alkhaldi HM, Alsakran WA, Magliyah MS.. Persistent Pupillary Dilation and Irreversible Mydriasis in HLA-B27-Associated Uveitis. Cureus. 2025;17(8):e89830. doi:10.7759/cureus.89830. PMID:40951017; PMCID:PMC12423723.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.