Ebola virus disease (EVD) is a zoonotic infection caused by a negative-sense single-stranded RNA virus belonging to the genus Ebolavirus in the family Filoviridae. The average fatality rate is approximately 50%.
Conjunctival injection (48–58%) is known as an acute ocular symptom, but the main ophthalmological concern is post-infection sequelae. The diverse symptoms in EVD survivors are collectively called post-Ebola virus disease syndrome (PEVDS). PEVDS includes arthritis, hearing loss, and neuropsychiatric disorders, and ophthalmic complications are among the most frequent sequelae1).
The 2013–2016 West African outbreak was the largest epidemic, with over 28,000 cases and approximately 11,000 deaths. A 2024 study of 112 EVD survivors in Sierra Leone found that uveitis was present in 21% (23/112) even at a median of 8 years after the outbreak, indicating a long-term burden of eye disease1).
QWhere does the Ebola virus hide in the eye?
A
The virus has been reported to be isolated as live virus particles from the aqueous humor, which is one of the “immune-privileged sites” where immune surveillance is limited. It has not been isolated from tears. Persistent infection can remain in the eye even after viremia has resolved.
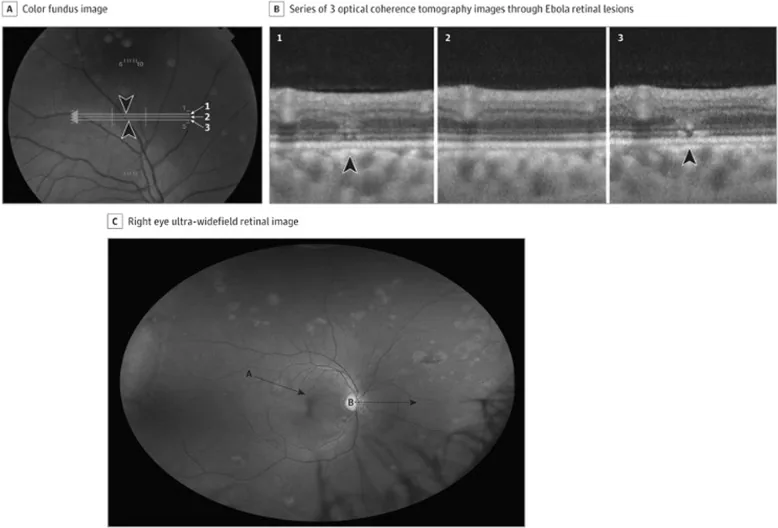
Ebola retinal lesions. A Colour fundus image, B corresponding OCT images showing discontinuities in the outer retinal layers, C multiple non-pigmented lesions and associated perilesional areas of dark without pressure. Source: Steptoe et al. [18] (CC-BY License).
Ocular findings in PEVDS appear as past inflammation or current inflammatory changes.
Anterior Segment Findings
Conjunctival injection and corneal edema: Observed during the active phase of inflammation.
Keratic precipitates (KP): Granulomatous or non-granulomatous.
Anterior chamber cells and flare: Reflect the degree of inflammation.
Posterior synechiae: Formed by recurrent inflammation.
Heterochromia iridis: Observed in some cases.
Posterior Segment Findings
Vitreous opacities: Due to infiltration of inflammatory cells.
Retinal lesions: Non-pigmented, with surrounding “dark without pressure” areas. Peripapillary lesions show a curved shape along the horizontal raphe, avoiding the fovea.
In a cohort study in Sierra Leone, 39% of eyes with confirmed uveitis had visual acuity worse than 20/400 (WHO blindness threshold) 1). Posterior uveitis (57%) and panuveitis (29%) were the main types 1). Cataract (18%), corneal scarring (9%), and optic neuropathy (6%) were observed as secondary complications 1).
QWhen does uveitis after EVD typically develop?
A
It usually develops 3 to 8 weeks after discharge from EVD. In most cases, it presents as unilateral anterior uveitis, but posterior and panuveitis are also seen to some extent. Furthermore, it has been reported that the burden of eye disease persists even several years after infection 1).
Risk factors for uveitis after EVD include the following:
High viral load: The higher the viral load during the acute phase, the greater the risk of uveitis.
Red eye during the acute phase: Bilateral red eye during acute EVD infection is a predictor of uveitis.
Advanced age: Aging increases the risk.
Persistent infection of the virus in immune-privileged sites is also considered a major mechanism of ocular complications1). Ebola virus can persist in body fluids, including aqueous humor and semen, for a long time after systemic viremia has cleared.
Travel to sub-Saharan Africa, where EVD is endemic, is the greatest risk factor. Healthcare workers are also at high risk of infection.
The diagnosis of PEVDS-associated uveitis is made by confirming intraocular inflammation in patients with a history of EVD. Although most current literature reports anterior uveitis as the most frequent type, some studies report posterior uveitis as the most common.
Evaluation of posterior segment and vitreous opacity
OCT shows abnormalities in the outer retinal layer. Fundus photography typically reveals non-pigmented retinal lesions surrounded by areas of “dark without pressure.”
Serological tests and antigen detection: Diagnosis of EVD. RT-PCR, ELISA, and virus isolation are useful in the acute phase.
Anterior chamber fluid testing (RT-PCR for viral RNA detection): Used to confirm the presence of intraocular virus. Particularly important before cataract surgery, as it helps assess the risk of viral exposure during surgical invasion.
In a cohort in Sierra Leone, anterior chamber fluid, vitreous fluid, and conjunctival samples from 50 EVD survivors scheduled for cataract surgery were tested by RT-PCR at 19 and 34 months, and all were confirmed negative for Ebola virus RNA.
Treatment is performed stepwise based on the severity at the initial visit.
Topical steroids (eye drops): Administered 4 times daily to every hour. Adjusted according to the degree of inflammation.
Cycloplegics: Used to prevent posterior synechiae and relieve eye pain.
Oral steroids (e.g., prednisone): Considered when vision is significantly reduced or inflammation worsens.
Intravitreal steroid injection: May be used for inflammation management.
There have been reports of antiviral drugs (oral favipiravir) used in combination with steroids, but it is unclear whether they contributed to disease resolution. To date, there are no reports of immunomodulatory drugs being used in the management of chronic Ebola-associated uveitis, and their role is unknown.
The most common surgical intervention in PEVDS is cataract surgery. Cataracts in EVD survivors are often very advanced, with a high risk of complications. Caution is needed regarding potential contact with live virus particles during surgery, and appropriate infection control measures are essential.
Ebola virus initially infects antigen-presenting cells (APCs) such as macrophages, Kupffer cells, and dendritic cells, and then disseminates throughout the body via the blood and lymphatic systems. Subsequently, infection spreads to fibroblasts, endothelial cells, hepatocytes, and adrenal cortical cells.
Viral infection of APCs causes immune dysregulation, leading to the release of large amounts of inflammatory and vasodilatory chemokines. Ultimately, endothelial dysfunction and coagulopathy lead to hypotension, shock, and multi-organ failure.
In the eye, persistent viral latency in immune-privileged sites such as the aqueous humor is considered a major mechanism of ophthalmic complications 1). Live virus particles have been isolated from the aqueous humor but not from tears.
A meta-analysis by Mandizadza et al. (2024) proposed a mechanism by which Ebola virus accumulates in immune-privileged sites (testes, central nervous system, intraocular fluid) and causes inflammation and direct tissue damage upon reactivation. Persistent infection of the virus in intraocular fluid and the central nervous system may cause ophthalmic and neurological symptoms 1).
It has also been suggested that the strong immune response (cytokine storm) caused by Ebola virus during acute infection may leave tissue damage and form a basis for long-term inflammation 1).
7. Latest Research and Future Prospects (Research-stage Reports)
Following the 2014 outbreak, vaccine development accelerated. On December 19, 2019, the U.S. FDA approved the rVSV-ZEBOV vaccine (brand name Ervebo) for the prevention of EVD in individuals aged 18 years and older. The widespread use of this vaccine may lead to a future reduction in the incidence of ophthalmic complications after EVD.
In a randomized controlled trial of EVD patients in the Democratic Republic of the Congo, MAb114 and REGN-EB3 were shown to be superior to ZMapp and remdesivir in acute treatment. The widespread use of these therapies has led to increased survival, making management of ophthalmic sequelae a more important issue.
A study in Sierra Leone showed that the burden of eye disease persists even at a median of 8 years after the EVD outbreak 1). The establishment of long-term ophthalmic care systems in affected regions has emerged as an important public health challenge.
Mandizadza OO, Phebeni RT, Ji C.. Prevalence of somatic symptoms among Ebola Virus Disease (EVD) survivors in Africa: a systematic review and meta-analysis. BMC Public Health. 2024;24(1):1511. doi:10.1186/s12889-024-19013-8. PMID:38840082; PMCID:PMC11155043.
Yeh S, Shantha JG, Hayek B, Crozier I, Smith JR. Clinical Manifestations and Pathogenesis of Uveitis in Ebola Virus Disease Survivors. Ocul Immunol Inflamm. 2018;26(7):1128-1134. PMID: 29993303.
Nabi W, Merle H, Abroug N, Jean-Charles A, Ksiaa I, Jelliti B, et al. [Viral uveitis in the tropics]. J Fr Ophtalmol. 2024;47(10):104342. PMID: 39509945.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.