Human T-cell Lymphotropic Virus type 1 (HTLV-1) is a virus belonging to the Retroviridae family, first discovered by Poiesz et al. in 1980. It causes adult T-cell leukemia/lymphoma (ATL), HTLV-1 associated myelopathy (HAM/TSP), arthropathy (HAAP), bronchiolitis (HAB), and uveitis (HTLV-1 associated uveitis; HAU)3).
HAU is a granulomatous or non-granulomatous uveitis occurring in HTLV-1 carriers, characterized mainly by vitreous opacities and retinal vasculitis. It is one of the important ophthalmic complications of HTLV-1 infection.
Epidemiology:
It is estimated that approximately 20 million people worldwide are infected, and the majority remain asymptomatic carriers throughout their lives.
In Japan, there is a regional concentration in the southwestern areas such as Kyushu, Okinawa, and southern Shikoku.
About 0.1% of HTLV-1 carriers develop ocular inflammation (nonspecific anterior uveitis and mild to moderate vitreous opacities) 4).
The prevalence of HAU is 112.2 per 100,000 carriers, slightly higher than that of HAM/TSP 5).
The male-to-female ratio is approximately 2:3, with a slight female predominance, and unilateral involvement is slightly more common.
According to the national epidemiological survey based on the Uveitis Clinical Practice Guidelines (2019), HAU accounted for 1.5% of all uveitis cases in the 2002 survey (5.1% in the Kyushu region) and 28 cases (0.7%) in the 2009 survey 2).
HAU can occur in combination with HAM/TSP or as the only sign of HTLV-1 infection. In cases with HAM/TSP, it tends to be more frequent in patients with earlier onset than in those with severe motor impairment. It also frequently coexists with hyperthyroidism.
Endemic areas also exist in Latin America, such as Colombia, and a report from Peru indicates that 29.4% of all intermediate uveitis cases (45.5% in those aged 50 and older) were HTLV-1-related 1).
QWhat kind of patients in Japan should be suspected of having HTLV-1-associated uveitis?
A
Suspect in patients from or residing in Kyushu, Okinawa, or southern Shikoku who present with uveitis predominantly characterized by vitreous opacity, when other known causes (such as sarcoidosis or intermediate uveitis) have been ruled out. Also consider HTLV-1 screening if hyperthyroidism or HAM/TSP (spastic paralysis, urinary disorders, etc.) are present.
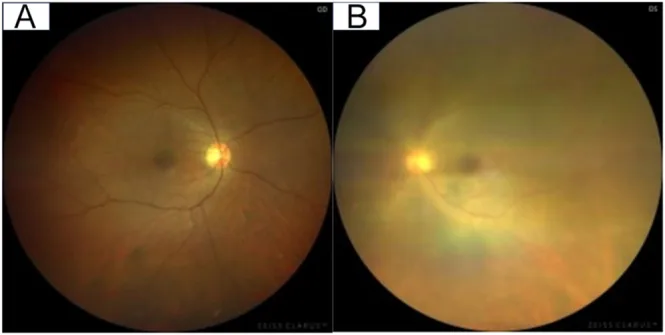
Kasamatsu D, et al. HTLV-1-associated uveitis mimicking thyroid-associated ophthalmopathy during antithyroid therapy: a diagnostic pitfall and management challenge. Endocrinol Diabetes Metab Case Rep. 2026. Figure 3. PMCID: PMC13052792. License: CC BY.
Comparison of right and left fundus photographs shows that in the active eye, the optic disc and retinal vessels are blurred due to vitreous opacity. This image demonstrates typical findings of intraocular inflammation seen in HTLV-1-associated uveitis.
Anterior granulomatous or non-granulomatous uveitis: Characterized by white granular keratic precipitates (KP) and iris nodules.
Corneal opacity, scarring, and neovascularization: Seen in chronic and severe cases.
Dry keratoconjunctivitis: May occur as an anterior segment complication.
Posterior Segment Findings
Vitreous opacities (veil-like, cord-like, or granular): Characteristic of HAU. A major cause of visual impairment.
White granular deposits around retinal blood vessels (retinal vasculitis): Particularly observed around the optic disc and along vascular arcades1).
Exudative retinochoroidal changes: Rarely observed in one or both eyes.
Retinal degeneration, retinal hemorrhage, epiretinal membrane, optic atrophy: May occur in severe or chronic cases.
Most infiltrating cells in HAU eyes are lymphocytes (predominantly CD3+ T cells), and cytokine production by HTLV-1-infected T cells triggers inflammation9). Veil-like vitreous opacities are an important diagnostic finding and should be considered in the differential diagnosis from sarcoidosis and intermediate uveitis5).
In a Colombian case series, severe cases presenting as intermediate and posterior uveitis showed extensive peripheral retinal degeneration, macular edema, and widespread retinal neovascularization1). Retinal photocoagulation (laser retinal ablation) may be necessary for severe retinal lesions.
QShould HTLV-1-associated uveitis be suspected if vitreous opacities are present?
A
For diseases primarily presenting with vitreous opacities, differentiation from sarcoidosis and intermediate uveitis is particularly important. HTLV-1 serological testing should be actively performed in individuals from endemic areas (such as Kyushu and Okinawa) or those with the above systemic complications.
HTLV-1 is a retrovirus that infects T lymphocytes (CD4+ T cells). The virus does not infect ocular tissues themselves; rather, the immune response triggered by infected T cells is central to the pathogenesis of HAU 9).
Main routes of infection:
Vertical transmission from mother to child (mainly through breastfeeding): The most important route of infection. The transmission rate is 20%, depending on HTLV-1 proviral load, maternal-child HLA class I compatibility, and duration of breastfeeding. Intrauterine and intrapartum infections are also possible.
Sexual intercourse (mainly with higher efficiency from male to female).
Blood contact and blood transfusion (the most efficient route of infection).
Risk factors:
Residence or origin in endemic areas (Kyushu, Okinawa, southern Shikoku, Caribbean countries, Central and South America, Central Africa, Melanesia).
Increased carrier prevalence in women aged 40 years and older.
ATL progression risk is 2–4% in infected individuals, HAM/TSP progression risk is 1–4%. Lifetime risk of associated inflammatory and autoimmune syndromes (uveitis, dermatitis, alveolitis, arthritis, nephritis, myositis, etc.) is approximately 10%1).
There are no definitive diagnostic criteria; diagnosis is made by exclusion 2).
Diagnostic Requirements:
Positive HTLV-1 serum antibody (confirmed by Western blot)
Exclusion of uveitis due to known causes (e.g., HSV, VZV, cytomegalovirus, tuberculosis, syphilis, toxoplasmosis, sarcoidosis, Behçet’s disease, multiple sclerosis)
Check for the presence of HTLV-1-related systemic diseases (ATL, HAM/TSP)
Detection of HTLV-1 proviral DNA by PCR in aqueous humor or peripheral blood samples also provides diagnostic evidence. In almost all cases of HAU patients, HTLV-1 proviral DNA is detected in the aqueous humor9). It has been found that even in HTLV-1-positive patients with uveitis due to other causes, the DNA is not detected, supporting the intraocular involvement of infected T cells.
HAU was first reported by Mochizuki et al. in 1992 3, 4). Subsequently, Nakao et al. described the clinical features in Kyushu in detail 5), and Yoshimura et al. clarified the immunological characteristics 6). Since the 1990s, a Japanese group led by Kamoi and Mochizuki has systematized the pathology, diagnosis, and treatment of HAU 7, 8, 10).
QWhat systemic examinations are necessary when HAU is diagnosed?
A
When HAU is diagnosed or strongly suspected, screening for ATL (adult T-cell leukemia) and HAM/TSP (myelopathy) is important. Specifically, perform peripheral blood leukocyte differential, LDH, soluble IL-2 receptor (screening for ATL), neurological evaluation (spastic paralysis, urinary disorders, etc., for HAM/TSP symptoms), and thyroid function tests (frequently associated with HAU). Since HTLV-1-related diseases involve multiple organs, collaboration with hematology, neurology, and internal medicine is recommended.
HAU responds well to systemic or local administration of steroids, and remits within weeks to months. Treatment intensity should be tailored to the degree of intraocular inflammation.
HAU responds well to steroids5, 6), but often relapses upon dose reduction or discontinuation. In severe cases in Colombia, immunomodulatory therapy (including cyclophosphamide) has been reported1).
Prognosis:
The initial prognosis is good in most cases, but recurrence occurs in about 60% of patients5). The average interval between recurrences is approximately 16 months1). Some reports indicate that over 90% of cases recur within 3 years1). Serious complications may include chorioretinal degeneration, glaucoma, and steroid-induced cataract1).
QHow can recurrence of HAU be reduced?
A
Currently, there is no established antiviral therapy against HTLV-1, and reliable means of preventing recurrence are limited. In case of recurrence, restarting or increasing steroids is the basic approach. Regular assessment of intraocular pressure and lens is important while monitoring for complications associated with long-term steroid therapy (steroidglaucoma, cataract). In cases complicated with HAM/TSP, collaboration with a neurologist is necessary.
6. Pathophysiology and Detailed Mechanism of Onset
HTLV-1 is a retrovirus that infects T lymphocytes (mainly CD4+ T cells) and does not directly infect ocular tissues8). Intraocular inflammation in HAU is caused by immune reactions mediated by HTLV-1-infected T cells.
Intraocular mechanism:
Cells floating in the anterior chamber are lymphocytes (mostly CD3+ T cells, with a few macrophages)9). PCR analysis detects HTLV-1 proviral DNA in almost all HAU patients, but not in uveitis patients due to other causes even if HTLV-1 positive. This indicates that infected T cells are directly involved in the pathogenesis of uveitis9).
HTLV-1-infected CD4+ T cell clones derived from infiltrating cells in HAU eyes produce large amounts of the following inflammatory cytokines:
IL-1α, IL-2, IL-3, IL-6, IL-8, IL-10
TNF-α, GM-CSF, IFN-γ
These cytokines induce immune responses and inflammation in the eye9).
Correlation between viral load and inflammation:
HTLV-1 proviral load in HAU patients is significantly higher than in asymptomatic carriers without uveitis10). The proviral load in peripheral blood mononuclear cells correlates with the intensity of intraocular inflammation. This relationship suggests the possibility of controlling inflammation through therapeutic intervention (reducing viral load).
The mechanism of posterior segment lesions (retinal vasculitis, exudative changes) is thought to involve HTLV-1-infected T cells producing a wide range of cytokines within the eye, leading to damage to retinal vascular endothelial cells and increased vascular permeability 7).
7. Latest Research and Future Perspectives (Reports at Research Stage)
Since HTLV-1 proviral load correlates with intraocular inflammation severity in HAU, reducing viral load has attracted attention as a therapeutic target 10). Although no HTLV-1 therapeutic drugs are currently approved, research on the application of reverse transcriptase inhibitors (e.g., zidovudine) is progressing.
Vaccine development is considered technically feasible, but no usable product currently exists. An approach combining infection prevention in endemic areas, especially blocking vertical transmission (mainly through breastfeeding) with promotion of alternative feeding (formula milk), is considered important 1).
In Latin American countries such as Colombia, HTLV-1 infection is poorly recognized as a “neglected infection,” and the actual status of HAU is not fully understood 1). There is a need to establish a diagnostic protocol that incorporates HTLV-1 serological testing as part of the differential diagnosis for patients with idiopathic uveitis. Kamoi (2023) reported a comprehensive review of ocular complications in HTLV-1 carriers and emphasized the importance of regular ophthalmologic screening 10).
Manabu Mochizuki, Kazunari Yamaguchi, Kiyoshi Takatsuki, Toshiki Watanabe, Shigeo Mori, Kazuo Tajima. HTLV-I and uveitis. The Lancet. 1992;339(8801):1110. doi:10.1016/0140-6736(92)90699-4.
Mochizuki M, Watanabe T, Yamaguchi K, Yoshimura K, Nakashima S, Shirao M, Araki S, Takatsuki K, Mori S, Miyata N.. Uveitis associated with human T-cell lymphotropic virus type I. Am J Ophthalmol. 1992;114(2):123-129. doi:10.1016/s0002-9394(14)73974-1. PMID:1642286.
Nakao K, Ohba N.. Clinical features of HTLV-I associated uveitis. Br J Ophthalmol. 1993;77(5):274-279. doi:10.1136/bjo.77.5.274. PMID:8100446; PMCID:PMC504504.
Yoshimura K, Mochizuki M, Araki S, Miyata N, Yamaguchi K, Tajima K, Watanabe T.. Clinical and immunologic features of human T-cell lymphotropic virus type I uveitis. Am J Ophthalmol. 1993;116(2):156-163. doi:10.1016/s0002-9394(14)71279-6. PMID:8352299.
Kamoi K, Mochizuki M. HTLV-1 uveitis. Front Microbiol. 2012;3:270.
Terada Y, Kamoi K, Komizo T, Miyata K, Mochizuki M.. Human T Cell Leukemia Virus Type 1 and Eye Diseases. J Ocul Pharmacol Ther. 2017;33(4):216-223. doi:10.1089/jop.2016.0124. PMID:28263674.
Ono A, Mochizuki M, Yamaguchi K, Miyata N, Watanabe T. Immunologic and virologic characterization of the primary infiltrating cells in the aqueous humor of human T-cell leukemia virus type-1 uveitis. Accumulation of the human T-cell leukemia virus type-1-infected cells and constitutive expression of viral and interleukin-6 messenger ribonucleic acids. Investigative ophthalmology & visual science. 1997;38(3):676-89. PMID:9071222.
Kamoi K. Uveitis and Ocular Complications in Human T-Cell Lymphotropic Virus Type 1 Carrier. Viruses. 2023;15(10):2024.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.