Asthenopia
Eye fatigue/heaviness: Worsens with prolonged near work
Blurred vision: Can occur both at distance and near
Eye pain/discomfort: Perceived as persistent dull pain
Diplopia (rare): Appears when accompanied by convergence insufficiency

Asthenopia refers to a set of nonspecific symptoms including eye fatigue, pain, blurred vision, headache, nausea, and sometimes vomiting that occur simply from looking at objects. Unlike simple “tired eyes,” it is a severe condition that does not improve with rest and is caused by organic or functional abnormalities of the eyes or the whole body. ICD-10 code is H53.1.
In the modern era where digital devices are essential, subtypes called computer vision syndrome (CVS) and digital eye strain (DES) are rapidly increasing. The TFOS (Tear Film & Ocular Surface Society) defines DES as “the development or exacerbation of recurrent ocular symptoms and signs specifically related to viewing digital device screens” 5). CVS refers to a variety of symptoms ranging from ocular symptoms (tired eyes, blurred vision, dry eye) to musculoskeletal symptoms (neck and shoulder pain) and neurological symptoms (headache) 7). “Technostress eye syndrome (IT eye syndrome)” that occurs during VDT work is a characteristic condition mainly involving dry eye due to decreased blinking and autonomic nervous system disorders.
Prevalence trends:
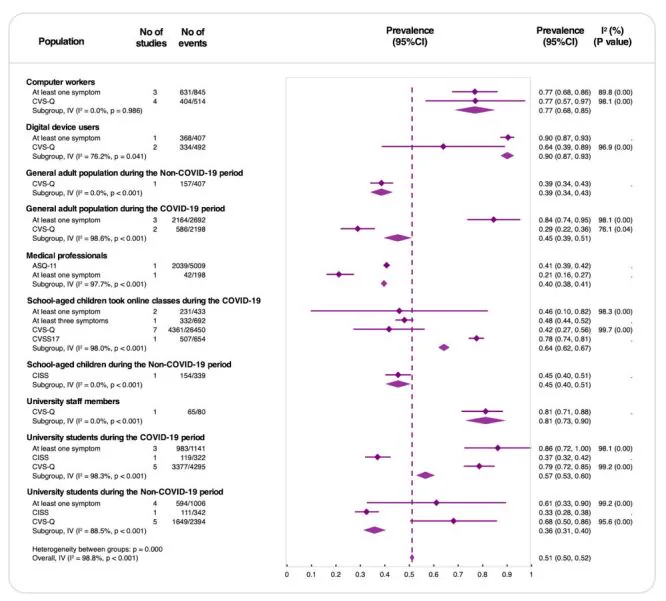
A systematic review and meta-analysis of 63 studies and 60,589 individuals by Song et al. reported an overall prevalence of asthenopia of 51% (95% CI: 50–52%) 1). It was high among digital device users (90%) and computer workers (77%), and during the COVID-19 pandemic, it increased from 45% to 64% in school-age children and from 36% to 57% in university students 1). The global prevalence of digital eye strain is approximately 66% (95% CI: 59–74%), reaching 74% (95% CI: 66–81%) during COVID-19 17).
Classification of causes:
The causes of asthenopia can be broadly classified into four types: accommodative, optical, muscular, and neurogenic.
| Classification | Main causes |
|---|---|
| Accommodative | Accommodative load due to refractive error or presbyopia, accommodative spasm, accommodative weakness |
| Optical | Inappropriate spectacle correction (undercorrection, overcorrection, poor anisometropia correction) |
| Muscular | Ocular misalignment (strabismus, heterophoria), convergence insufficiency |
| Neurogenic | Systemic diseases, psychological factors, autonomic nervous system disorders due to VDT work |
“Tired eyes” refers to a transient condition that resolves with rest. Asthenopia is a severe condition that does not improve with rest and is distinguished as an indefinite syndrome based on underlying conditions such as refractive errors, ocular misalignment, and systemic diseases.
Subjective symptoms of asthenopia include a variety of complaints involving both ocular and systemic symptoms.
Symptom frequency from meta-analysis1):
In a meta-analysis of 63 studies involving 60,589 participants by Song et al. (2026), the following symptoms were reported.
| Symptom | Category | Notes |
|---|---|---|
| Blurred vision or difficulty focusing | Ocular | One of the most frequent complaints |
| Eye fatigue or heaviness | Ocular | Common among all digital device users |
| Dry eye sensation | Ocular (dry eye) | Mainly due to decreased blink rate |
| Eye pain/discomfort | Ocular | Persistent dull pain |
| Headache (frontal) | Systemic | Related to accommodative and convergence effort |
| Neck and shoulder stiffness | Systemic (musculoskeletal) | Triggered by improper posture and working distance |
| Diplopia | Ocular | When accompanied by convergence insufficiency |
| Photophobia | Ocular | Related to ocular surface disorders |
Blurred vision, haziness, dryness, and a heavy sensation in the eyes are also frequently reported. In severe cases, blepharospasm may occur. True treatment of asthenopia involves identifying the cause and preventing its onset; it is important to distinguish it from simple eye strain.
Four-category classification of digital eye strain (DES)8):
Asthenopia
Eye fatigue/heaviness: Worsens with prolonged near work
Blurred vision: Can occur both at distance and near
Eye pain/discomfort: Perceived as persistent dull pain
Diplopia (rare): Appears when accompanied by convergence insufficiency
Dry eye-related symptoms
Dryness: Mainly due to decreased blink rate
Foreign body sensation/burning: Caused by tear film breakup
Tearing: Due to reflex lacrimation
Photophobia: Appears with ocular surface disorders
Exacerbation of Pre-existing Eye Disease
Manifestation of Uncorrected Refractive Error: Mild astigmatism or presbyopia amplifies symptoms
Headache: Especially common in the frontal region
Difficulty Focusing: Particularly noticeable in presbyopia
Musculoskeletal Symptoms
Neck and Shoulder Pain: Caused by poor posture
Lower Back Pain: Related to improper screen positioning
Wrist and Finger Pain: Occurs with prolonged keyboard use
Characteristic Findings of Technostress Eye Syndrome:
During VDT work, blinking frequency clearly decreases, and combined with office dryness, leads to functional dry eye. After work, compensatory increase in blinking is observed. The near response (accommodation, miosis, convergence) is normally triggered simultaneously during near vision, but after VDT work, this coordination breaks down, causing inconsistency in the simultaneous triggering of the three elements.
If repeated eye dryness, fatigue, blurred vision, and headache occur after prolonged use of digital devices and improve when use is stopped, digital eye strain is likely. It can be assessed using standardized questionnaires such as the CVS-Q (Computer Vision Syndrome Questionnaire, score ≥6 indicates DES). If symptoms persist, it is important to see an ophthalmologist to check for refractive errors, accommodative disorders, and dry eye.
Eye strain is a multifactorial condition, resulting from a combination of ophthalmic, systemic, and environmental factors.
Ophthalmic Factors:
Systemic factors:
Environmental factors:
Risk and protective factors from meta-analysis (OR values) 1):
| Factor | OR (95% CI) | Classification |
|---|---|---|
| Air conditioner use | 23.02 (4.94–107.18) | Risk |
| Pre-existing eye disease | 2.59 (1.43–4.69) | Risk |
| Poor sitting posture | 2.02 (1.51–2.70) | Risk |
| Hyperopia | 1.56 (1.10–2.30) | Risk |
| Myopia | 1.51 (1.27–1.81) | Risk |
| Screen time (per 1-hour increase) | 1.15 (1.09–1.21) | Risk |
| Regular breaks | 0.21 (0.09–0.51) | Protective |
| Good sleep quality | 0.24 (0.20–0.30) | Protective |
| Computer use knowledge | 0.20 (0.13–0.30) | Protective |
| Anti-glare filter | 0.34 (0.19–0.64) | Protective |
Specific risk factors for digital eye strain include short viewing distance (OR 4.24), poor ergonomics (OR 3.87), and lack of breaks (OR 2.24)15). When the screen is positioned above eye level, the exposed ocular surface area increases, worsening dry eye symptoms5). In a meta-analysis of computer workers, VDT usage time, work environment, and spectacle correction status were identified as major determinants of prevalence14).
Cases of hyperopic shift and asthenopic symptoms after COVID-19 infection have been reported, suggesting a decline in the ciliary muscle’s ability to maintain accommodation2).
Each additional hour of screen time increases the risk of eye strain by OR 1.15 (95% CI: 1.09–1.21)1). Conversely, taking regular breaks reduces the risk to OR 0.21. Combining screen time limits with regular breaks is important.
The most important aspect of diagnosing eye strain is a detailed history. Carefully inquire about VDT usage time, work environment, timing of symptom onset, spectacle prescription history, and use of medications such as psychotropic drugs or antihistamines.
Essential ophthalmic examinations:
| Examination | Purpose | Key points |
|---|---|---|
| Distance and near visual acuity test | Confirmation of refractive error | Measure all at 5m, near (30cm), and intermediate distance (50cm) |
| Refraction test | Confirmation of appropriate correction | Autorefractor + subjective refraction. Cyclopentolate eye drops if needed |
| Accommodation function test | Evaluation of accommodative amplitude and status | Near point measurement, repeated measurement, accommodation function analyzer (HFC analysis) |
| Eye position test | Evaluation of strabismus and phoria | Alternate cover test, prism cover test |
| Stereopsis test | Evaluation of binocular vision function | TNO, Titmus |
| Dry eye test | Evaluation of ocular surface damage | TBUT, Schirmer test, fluorescein staining |
| Slit-lamp microscopy | Exclusion of anterior segment diseases | Includes evaluation of meibomian gland dysfunction |
| Fundus examination | Exclusion of glaucoma and fundus diseases | Assessment of optic disc findings and visual field abnormalities |
It has been pointed out that tear film instability can be a major cause of visual fatigue3), and evaluation of meibomian gland dysfunction is also important.
Assessment using questionnaires:
Standardized questionnaires include the following8)12).
| Questionnaire | Number of items | Diagnostic criteria |
|---|---|---|
| CVS-Q (Computer Vision Syndrome Questionnaire) | 16 symptoms | Score ≥6 indicates DES |
| CVSS17 (Computer Vision Symptom Scale) | 17 items | Based on Rasch model |
| DESQ (Digital Eye Strain Questionnaire) | Multiple items | Covers all digital devices |
Objective tests (for research/specialized facilities)5):
Diseases to be excluded:
It is necessary to exclude diseases that present symptoms similar to asthenopia, such as angle-closure glaucoma, uveitis, and optic neuritis. Pay particular attention to the following points.
Treatment of asthenopia is fundamentally based on a multifaceted approach according to the cause. The most important aspect is to identify and eliminate the cause; symptomatic treatment alone leads to recurrence. Treatment is performed in the following order of priority:
Refractive correction and orthoptic correction
Proper spectacle prescription: The most important means of treating asthenopia. Accurately correct hyperopia, astigmatism, and anisometropia. Both undercorrection and overcorrection can cause asthenopia.
Contact lens prescription: For large anisometropia, contact lenses are more effective than spectacles in reducing aniseikonia.
Prism spectacles: Prism spectacles are effective for heterophoria of about 10 prism diopters (Δ). For vertical deviation, even small angles have a narrow fusion range, so active treatment should be considered.
Vision training: Training for convergence insufficiency and binocular vision dysfunction. Surgery is indicated for large-angle ocular misalignment.
VDT Environment Improvement and Behavioral Changes
Regular breaks: Take a 10-15 minute break every hour and try to look at distant objects.
20-20-20 rule: Every 20 minutes, look at something 20 feet (about 6 m) away for 20 seconds 13).
Monitor distance and position: Keep the distance between eyes and computer at 40-70 cm. Position the screen so that your gaze is slightly downward.
Lighting and environment: Avoid direct sunlight and ensure sufficient indoor lighting. Avoid direct airflow from air conditioning or heating, and ensure proper ventilation. Humidity control is also important.
Medication and Nutritional Therapy
Artificial tears: Soft Santear ophthalmic solution, 2-3 drops per dose, 5-6 times daily
Moisturizing eye drops: Hyalein ophthalmic solution (0.1%), 1 drop per dose, 5-6 times daily + Mucosta ophthalmic solution UD (2%) or Diquas ophthalmic solution (3%), 1 drop per dose, 5-6 times daily
Treatment for accommodative spasm: Mydrin M ophthalmic solution (0.4%), once daily at bedtime (to relieve ciliary muscle hypertonicity)
Eye drops for asthenopia: Sancoba ophthalmic solution (0.02%), 3-5 times daily
Omega-3 fatty acid supplementation: The only oral nutritional intervention with high-quality evidence shown in a systematic review by TFOS 6)
Blinking exercise: Repeat a set of closing eyes for 2 seconds twice, then forcefully closing eyelids for 2 seconds 11). Effective as conscious blinking practice during VDT work.
Current randomized controlled trials have not confirmed evidence that blue light blocking lenses significantly reduce symptoms of eye strain 5). The main causes of eye strain are accommodative fatigue, abnormal blinking, and environmental factors, not the wavelength characteristics of light. For prevention, it is recommended to prioritize the 20-20-20 rule, proper refractive correction, and optimization of the work environment.
The mechanisms of eye strain vary depending on the cause, and multiple mechanisms often combine.
Mechanisms due to refractive error and improper correction:
Squinting in an uncorrected state or improper refractive correction can lead to accommodative spasm or accommodative insufficiency, or conversely, accommodative paralysis. These accommodative abnormalities are major causes of eye strain and can progress into a negative spiral.
Accommodative mechanisms (technostress eye syndrome):
The mechanism of accommodative spasm due to VDT work and prolonged smartphone use is as follows. Continuous near work causes sustained contraction and tension of the ciliary muscle, making relaxation difficult (accommodative spasm). If it becomes more severe, accommodative spasm leads to pseudomyopia-like distance vision impairment. Accommodative function analysis (Fk-map) shows a pattern of accommodative spasm to spasm with high HFC values for near targets. In this state, eye strain tends to become chronic. Improvement can be achieved by instilling a cycloplegic agent (Mydrin M) before bedtime to relax the ciliary muscle.
Convergence and binocular vision mechanisms:
In convergence insufficiency with accommodative insufficiency, both accommodative convergence and fusional convergence are insufficient, causing diplopia and eye strain during near vision. Prolonged near use of digital devices requires sustained accommodative effort, leading to decreased accommodative amplitude, recession of the near point of convergence, and increased accommodative lag 9)10).
Mechanisms of abnormal blinking and ocular surface disorders:
During digital device use, the blink rate decreases and incomplete blinks increase 5)8). The normal blink rate is 15-20 times per minute, but it significantly decreases during screen viewing. Decreased blink rate promotes tear evaporation, increases tear osmolarity, and induces ocular surface dryness and inflammation. Tear film instability is one of the main causes of visual fatigue 3).
Nutritional and metabolic mechanisms:
DHA (docosahexaenoic acid) accounts for approximately 50% of the phospholipids in retinal photoreceptors, and supplementation with omega-3 polyunsaturated fatty acids (PUFAs) has been suggested to be effective in reducing oxidative stress in the retina and ocular surface 4).
Mechanism after COVID-19:
It has been reported that after COVID-19 infection, decreased parasympathetic innervation leads to reduced ciliary muscle tone, causing a hyperopic shift in refraction and symptoms of asthenopia 2). In three cases (a 31-year-old woman, a 25-year-old man, and a 22-year-old man), hyperopic shifts were observed, and symptoms improved with appropriate spectacle correction. This mechanism is thought to result from damage to the autonomic and parasympathetic nervous systems as a neurological sequela of COVID-19, and attention should be paid to changes in refractive status in the ophthalmological evaluation of long COVID patients.
Asthenopia and tear film stability:
Tear film instability is one of the main causes of visual fatigue 3). Without a normal tear film, the optically uniform ocular surface cannot be maintained, leading to fluctuations and blurring of vision. Decreased blink rate during digital device use is a major mechanism causing this tear film instability. Evaporative dry eye due to meibomian gland dysfunction (MGD) is an important comorbidity that worsens asthenopia, and active evaluation and treatment are necessary.
Cases have been reported in which hyperopic shift and symptoms of asthenopia appeared after COVID-19 infection, and it is thought that decreased ability of the ciliary muscle to maintain accommodation is involved 2). Symptoms may improve with appropriate refractive correction.
Proposal for a unified diagnostic definition:
There is no internationally agreed diagnostic definition for asthenopia, making comparison between studies difficult. A meta-analysis by Song et al. (2026) proposes the following unified diagnostic criteria 1).
Proposed definition: “A syndrome primarily caused by visual tasks, presenting with one or more symptoms related to the eyes or vision (such as eye fatigue, blurring, pain, etc.), which are partially or completely relieved by rest.” If this definition is standardized, it is expected to improve the quality of future epidemiological and interventional studies.
Future directions for treatment and management:
Current treatment for asthenopia is mainly symptomatic, but evolution in the following directions is expected:
Global trends in prevalence13)17):
| Population | Prevalence |
|---|---|
| World (normal, DES) | 66% (95% CI: 59–74%) |
| During COVID-19 (DES) | 74% (95% CI: 66–81%) |
| Non-students (during COVID) | 82% |
| Students (during COVID) | 70% |
| All ages and overall asthenopia | 51% (95% CI: 50–52%) |
| Digital device users | 90% |
| Computer workers | 77% |
Impact on children:
DES is also called a “shadow pandemic” in children 16). The average screen time doubled from 1.9 hours to 3.9 hours before and after the COVID-19 pandemic, and the prevalence of DES in children reached 50.2%. Age 14 or older, male sex, and device use for more than 5 hours per day were identified as risk factors.
Potential of omega-3 fatty acid supplements:
Supplementation with omega-3 PUFAs may reduce oxidative stress on the ocular surface and improve visual fatigue through stabilization of the tear film 4). In a systematic review by TFOS, oral omega-3 fatty acid supplementation is positioned as the management method with the highest level of evidence 6).
Objective evaluation techniques for tear film stability:
Methods for objectively evaluating tear film stability are being developed 3). If this technology is applied clinically, it will enable objective diagnosis and monitoring of dry eye-related asthenopia. If non-invasive tear film evaluation (NIBUT: Non-Invasive Break-Up Time) during digital device use becomes widespread, it may be possible to track changes in the ocular surface before and after screen time in real time.
Impact of VR head-mounted displays:
VR (virtual reality) head-mounted displays impose a near-distance visual load different from conventional screens, raising concerns about effects on accommodation and vergence function. Development of DES monitoring and prevention systems using AI and wearable devices is also progressing.
Asthenopia and medical economics:
Asthenopia is closely associated with decreased productivity and increased healthcare costs worldwide. With the normalization of remote work after the COVID-19 pandemic, the economic significance of workplace measures against eye strain (ergonomic improvements, regular breaks, periodic eye exams) is being reassessed. Considering that each additional hour of screen time increases the risk by OR 1.15, investment in workplace environment improvements is likely to lead to long-term healthcare cost reductions 1).
Prevention programs for asthenopia:
The following measures are recommended for preventing eye strain in workplaces and schools:
Song F, Liu Y, Zhao Z, Shang X, Wang Y, Lai M, et al. Clinical manifestations, prevalence, and risk factors of asthenopia: a systematic review and meta-analysis. Journal of global health. 2026;16:04053. doi:10.7189/jogh.16.04053. PMID:41648943; PMCID:PMC12879263.
Thakur M, Panicker T, Satgunam P. Refractive error changes and associated asthenopia observed after COVID-19 infection: Case reports from two continents. Indian journal of ophthalmology. 2023;71(6):2592-2594. doi:10.4103/IJO.IJO_2581_22. PMID:37322686; PMCID:PMC10418019.
Watanabe M, Hirota M, Takigawa R, Kato K, Ikeda Y. Objective Evaluation of Relationship Between Tear Film Stability and Visual Fatigue [Response to Letter]. Clinical optometry. 2025;17:281-282. doi:10.2147/OPTO.S558482. PMID:40922902; PMCID:PMC12414455.
Duan H, Song W, Zhao J, Yan W. Polyunsaturated Fatty Acids (PUFAs): Sources, Digestion, Absorption, Application and Their Potential Adjunctive Effects on Visual Fatigue. Nutrients. 2023;15(11). doi:10.3390/nu15112633. PMID:37299596; PMCID:PMC10255902.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Wolffsohn JS, Lingham G, Downie LE, et al. TFOS Lifestyle: Impact of the digital environment on the ocular surface. Ocul Surf. 2023 Apr;28:213-252. doi:10.1016/j.jtos.2023.04.004. PMID:37062428.
Kahal F, Al Darra A, Torbey A. Computer vision syndrome: a comprehensive literature review. Future science OA. 2025;11(1):2476923. doi:10.1080/20565623.2025.2476923. PMID:40055942; PMCID:PMC11901492.
Pucker AD, Kerr AM, Sanderson J, Lievens C. Digital Eye Strain: Updated Perspectives. Clin Optom. 2024;16:249-261.
Barata MJ, Aguiar P, Grzybowski A, Moreira-Rosário A, Lança C. A Review of Digital Eye Strain: Binocular Vision Anomalies, Ocular Surface Changes, and the Need for Objective Assessment. Journal of eye movement research. 2025;18(5):39. doi:10.3390/jemr18050039. PMID:40989226; PMCID:PMC12452390.
Kaur K, Gurnani B, Nayak S, et al. Digital Eye Strain- A Comprehensive Review. Ophthalmol Ther. 2022;11:1655-1680.
Pavel IA, Bogdanici CM, Donica VC, Anton N, Savu B, Chiriac CP, et al. Computer Vision Syndrome: An Ophthalmic Pathology of the Modern Era. Medicina (Kaunas, Lithuania). 2023;59(2). doi:10.3390/medicina59020412. PMID:36837613; PMCID:PMC9961559.
Mylona I, Glynatsis MN, Floros GD, Kandarakis S. Spotlight on Digital Eye Strain. Clin Optom. 2023;15:29-36.
León-Figueroa DA, Barboza JJ, Siddiq A, Sah R, Valladares-Garrido MJ, Adhikari S, et al. Prevalence of computer vision syndrome during the COVID-19 pandemic: a systematic review and meta-analysis. BMC public health. 2024;24(1):640. doi:10.1186/s12889-024-17636-5. PMID:38424562; PMCID:PMC10902934.
Lema AK, Anbesu EW. Computer vision syndrome and its determinants: A systematic review and meta-analysis. SAGE open medicine. 2022;10:20503121221142402. doi:10.1177/20503121221142402. PMID:36518554; PMCID:PMC9743027.
Lem DW, Gierhart DL, Davey PG. Can Nutrition Play a Role in Ameliorating Digital Eye Strain? Nutrients. 2022;14(19):4005.
Bhattacharya S, Heidler P, Saleem SM, Marzo RR. Let There Be Light-Digital Eye Strain (DES) in Children as a Shadow Pandemic in the Era of COVID-19: A Mini Review. Frontiers in public health. 2022;10:945082. doi:10.3389/fpubh.2022.945082. PMID:36033797; PMCID:PMC9403324.
Anbesu EW, Lema DW. Prevalence of computer vision syndrome: a systematic review and meta-analysis. Sci Rep. 2023;13:1801.