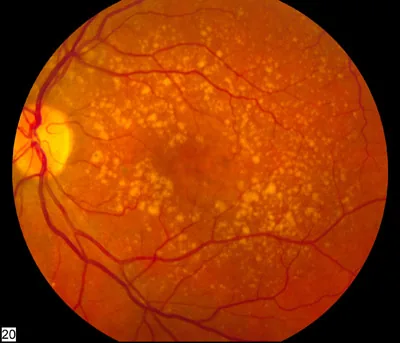
Right eye fundus photograph showing extensive accumulation of multiple pale yellow soft drusen in the macula, consistent with moderate age-related macular degeneration. This corresponds to the typical fundus finding of AMD, for which smoking is the greatest risk factor, as discussed in section “1. Relationship Between Smoking and Eye Diseases.”
Tobacco smoke contains over 4,000 chemical substances, among which cyanide, cadmium, nicotine, and free radicals cause various damages to ocular tissues. The odds ratio for AMD onset in current smokers is 2.0–4.0 (systematic review and meta-analysis)1), making it the strongest modifiable risk factor for AMD. For nuclear cataract, smoking of 20 pack-years or more increases the odds ratio to approximately 2.02).
There is a clear dose-response relationship between cumulative smoking amount (pack-years = number of cigarettes smoked per day ÷ 20 × years of smoking) and the risk of eye diseases1). After quitting smoking, the risk gradually decreases, but it may take more than 20 years to return to the same level as non-smokers3), so early smoking cessation provides the greatest benefit. Passive smoking (exposure to secondhand smoke) is associated with an increased risk of allergic diseases in children and adolescents4).
Nuclear cataract risk increases to OR approximately 2.0 with 20 pack-years or more2)
Risk decreases to near that of non-smokers 20 years after quitting3)
Passive smoking may also increase the risk of allergic diseases4)
QHow does smoking affect the eyes?
A
Smoking increases the risk of age-related macular degeneration by 2 to 4 times and the risk of nuclear cataract by about 2 times. The main mechanism is that oxidants, cyanide, and cadmium in tobacco smoke damage the retinal pigment epithelium and lens proteins. It is also an aggravating factor for dry eye, thyroid eye disease (TED), and diabetic retinopathy. In particular, the risk of developing eye disease in patients with Graves’ disease is about 7.7 times higher than in non-smokers. Passive smoking may also increase the risk of eye diseases, so improving the environment not only for the smoker but also for those around them is important.
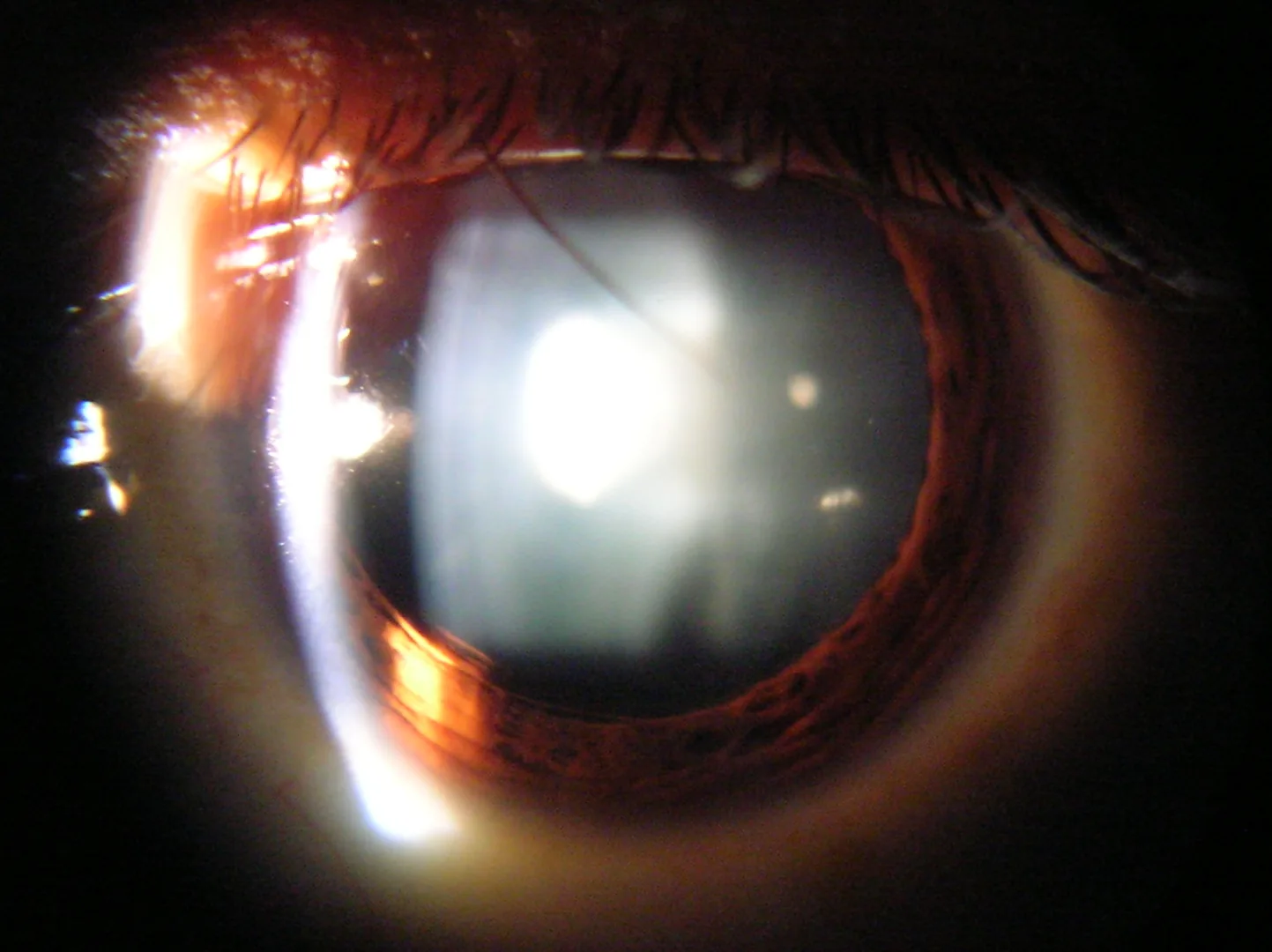
Slit-lamp microscopy image showing marked brownish opacification of the lens nucleus (nuclear cataract). This corresponds to the nuclear cataract caused by cyanide from smoking, discussed in the section “2. Eye diseases associated with smoking.”
The main eye diseases associated with smoking can be categorized into six types.
Age-related macular degeneration (AMD)
Risk of onset: OR for AMD in current smokers is 2.0–4.0 (meta-analysis)1)
Strong association with exudative AMD: Particularly strong association with exudative (neovascular) AMD5)
Dose-response relationship: Positive dose-response relationship with cumulative smoking amount (pack-years)1)
Effect of smoking cessation: Risk decreases to near that of non-smokers 20 years after quitting3)
Cataract
Nuclear cataract risk: OR approximately 2.0 for 20 pack-years or more2)
Association with posterior subcapsular cataract also reported6)
Mechanism: Disruption of disulfide bonds in lens proteins by cyanide leads to nuclear cataract
Effect of smoking cessation: Risk reduction observed after quitting2)
Dry Eye
Direct harmful effect: Tobacco smoke directly damages the tear film7)
Goblet cell damage: Thinning of the mucus layer due to damage to conjunctival goblet cells7)
Secondhand smoke environment may increase the risk of allergic diseases4)
Thyroid Eye Disease (TED)
Strongest environmental factor: Smoking is the strongest environmental factor for the onset and exacerbation of Graves’ ophthalmopathy8)
Risk of onset: OR for TED onset in smokers approximately 7.78)
After radioactive iodine treatment, risk of TED exacerbation is increased in smokers9)
Diabetic Retinopathy and Leber Hereditary Optic Neuropathy
Smoking triggers the onset in carriers of mitochondrial DNA mutations11)
Smoking exacerbates mitochondrial dysfunction, increasing the risk of onset11)
QWhat is the relationship between thyroid eye disease and smoking?
A
Smoking is the strongest environmental factor, increasing the risk of developing thyroid eye disease (TED) in patients with Graves’ disease by approximately 7.7 times. Smoking cessation has been shown to improve the effectiveness of TED treatment, and the risk of worsening eye disease after radioactive iodine therapy is also higher in smokers. Providing smoking cessation guidance before starting eye disease treatment (steroids, radiation therapy, orbital decompression) is a prerequisite for maximizing treatment efficacy.
The population attributable risk (PAR) of smoking for AMD is estimated to be approximately 25–30% 1)
A significant increase in cataract surgery risk among smokers has been confirmed in large cohort studies 6)
Secondhand smoke exposure has been reported to increase the risk of allergic diseases in children and adolescents 4)
Research on the ocular effects of electronic cigarettes (including heated tobacco products) is accumulating 12), and the establishment of evidence is awaited
External photograph of Graves’ disease (thyroid eye disease) showing marked bilateral proptosis and upper eyelid retraction. This corresponds to the clinical presentation of thyroid eye disease, for which smoking increases the risk of onset by approximately 7.7 times, as discussed in the section “4. Diagnosis and Screening.”
Active inquiry into smoking history is important in ophthalmology outpatient settings. It should be considered an essential item, especially during initial consultations for AMD and thyroid eye disease.
Quantification of smoking history:
Calculation of pack-years: (number of cigarettes smoked per day ÷ 20) × years of smoking
Confirm whether the patient is a current smoker, former smoker (with years since quitting), or never smoker
Also assess secondhand smoke exposure (at work and home)
Varenicline (Champix): α4β2 nicotinic receptor partial agonist. Standard treatment is 12 weeks13)
Collaboration with smoking cessation clinics: Utilize the insurance-covered 12-week smoking cessation treatment program (5 visits)14)
QDoes quitting smoking reduce eye risks?
A
Prospective cohort studies have shown that the risk of AMD significantly decreases 10 to 20 years after quitting smoking. However, the risk does not fully return to the level of non-smokers, and the earlier you quit, the greater the benefit. Risk reduction after quitting has also been observed for nuclear cataracts and thyroid eye disease. Especially during treatment for thyroid eye disease, quitting smoking improves treatment outcomes. From an ophthalmological perspective, smoking cessation is extremely important, and it is advisable to actively recommend the use of smoking cessation clinics (covered by insurance).
6. Pathophysiology and detailed mechanisms of onset
The main mechanisms by which smoking damages ocular tissues are broadly divided into four categories: oxidative stress, direct toxicity, immune dysregulation, and vascular damage.
It is estimated that a single puff of cigarette smoke produces approximately 10^15 free radicals15)
In mice exposed to cigarette smoke, RPE oxidative DNA damage, loss of basal infoldings, increased vacuolization, Bruch’s membrane thickening, and RPEapoptosis have been reported 15)
Nrf2 orchestrates the antioxidant response, and its response decline due to aging and smoking-related oxidative stress is a concern 15)
The synergistic effect of complement factor H (CFH) gene polymorphism (Y402H) and smoking significantly increases AMD risk 5)
Effects of e-cigarettes and heated tobacco products on the eyes:
Epidemiological studies evaluating the ocular effects of e-cigarettes and heated tobacco products (e.g., IQOS) are accumulating12)
Concerns exist regarding the impact on the ocular surface via nicotine and volatile organic compounds
Risk assessment compared to conventional tobacco is not yet established, so a cautious approach is necessary
Gene–environment interaction:
Interaction between CFH (Y402H) and ARMS2 (A69S) gene polymorphisms and smoking further increases AMD risk5)
Research on personalized smoking cessation interventions for genetically high-risk individuals is progressing
Smoking cessation intervention and AMD progression suppression:
Prospective cohort studies are underway to verify the effects of smoking cessation on suppressing AMD onset and progression
The combined effect of smoking cessation and AREDS supplements (vitamin C 500 mg, vitamin E 400 IU, zinc 80 mg, copper 2 mg, lutein 10 mg, zeaxanthin 2 mg) is also being evaluated.
Thirdhand smoke:
The impact of residual chemicals (thirdhand smoke) adhering to walls, clothing, and furniture on the ocular surface is attracting attention.
The association with ocular surface disorders in children and family members of smokers is a topic for future research.
AI-based estimation of smoking status from fundus photographs:
Studies using machine learning models to estimate smoking status from fundus photographs have been reported, and application to ophthalmic screening is expected.
Usha Chakravarthy, Tien Y Wong, Astrid Fletcher, Elisabeth Piault, Christopher Evans, Gergana Zlateva, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10(1). doi:10.1186/1471-2415-10-31.
Ye J, He J, Wang C, Wu H, Shi X, Zhang H, et al. Smoking and risk of age-related cataract: a meta-analysis. Investigative ophthalmology & visual science. 2012;53(7):3885-95. doi:10.1167/iovs.12-9820. PMID:22599585.
Khan JC, Thurlby DA, Shahid H, et al. Smoking and age related macular degeneration: the number of pack years of cigarette smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation. Br J Ophthalmol. 2006;90(1):75-80. doi:10.1136/bjo.2005.073643.
Saulyte J, Regueira C, Montes-Martinez A, Khudyakov P, Takkouche B. Active or passive exposure to tobacco smoking and allergic rhinitis, allergic dermatitis, and food allergy in adults and children: a systematic review and meta-analysis. PLoS Med. 2014;11(3):e1001611. PMCID: PMC3949681. doi:10.1371/journal.pmed.1001611.
Seddon JM, George S, Rosner B. Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: the US Twin Study of Age-Related Macular Degeneration. Archives of ophthalmology (Chicago, Ill. : 1960). 2006;124(7):995-1001. doi:10.1001/archopht.124.7.995. PMID:16832023.
Kelly SP, Thornton J, Edwards R, Sahu A, Harrison R. Smoking and cataract: review of causal association. Journal of cataract and refractive surgery. 2005;31(12):2395-404. doi:10.1016/j.jcrs.2005.06.039. PMID:16473237.
Moss SE, Klein R, Klein BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264-1268. doi:10.1001/archopht.118.9.1264.
Mark F. Prummel. Smoking and Risk of Graves’ Disease. JAMA. 1993;269(4):479. doi:10.1001/jama.1993.03500040045034.
Bartalena L, Marcocci C, Tanda ML, Manetti L, Dell’Unto E, Bartolomei MP, et al. Cigarette smoking and treatment outcomes in Graves ophthalmopathy. Annals of internal medicine. 1998;129(8):632-5. doi:10.7326/0003-4819-129-8-199810150-00010. PMID:9786811.
Cai J, Boulton M. The pathogenesis of diabetic retinopathy: old concepts and new questions. Eye (Lond). 2002;16(3):242-260. doi:10.1038/sj.eye.6700133. PMID: 12032713.
Kirkman MA, Yu-Wai-Man P, Korsten A, Leonhardt M, Dimitriadis K, De Coo IF, et al. Gene-environment interactions in Leber hereditary optic neuropathy. Brain : a journal of neurology. 2009;132(Pt 9):2317-26. doi:10.1093/brain/awp158. PMID:19525327; PMCID:PMC2732267.
Mehra D, Galor A. Digital Screen Use and Dry Eye: A Review. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2020;9(6):491-497. doi:10.1097/APO.0000000000000328. PMID:33181547.
Fiore MC, Jaén CR, Baker TB, et al. Treating tobacco use and dependence: 2008 update. Clinical practice guideline. Rockville, MD: U.S. Department of Health and Human Services; 2008.
JCS Joint Working Group. Guidelines for smoking cessation (JCS 2010): digest version. Circ J. 2012;76(4):1024-1043.
Cano M, Thimmalappula R, Fujihara M, Nagai N, Sporn M, Wang AL, et al. Cigarette smoking, oxidative stress, the anti-oxidant response through Nrf2 signaling, and Age-related Macular Degeneration. Vision research. 2010;50(7):652-64. doi:10.1016/j.visres.2009.08.018. PMID:19703486; PMCID:PMC3575185.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.


{kind=link}
{kind=link}
{kind=link}