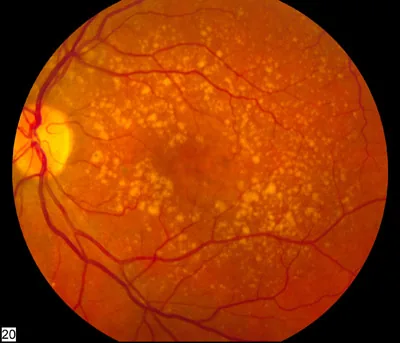
National Eye Institute, National Institutes of Health. Intermediate age-related macular degeneration fundus photograph. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Intermediate_age_related_macular_degeneration.jpg. License: CC BY (Public Domain, U.S. federal government work).
Numerous medium to large drusen (yellow-white deposits) scattered in the macula, showing typical fundus findings of intermediate AMD. This corresponds to the drusen findings of intermediate AMD (AREDS category 3) that were the subject of the AREDS study discussed in the section “1. Relationship between supplements and eye diseases.”
The field examining the scientific evidence of nutrients and supplements for the prevention and progression suppression of eye diseases is attracting attention. In particular, large-scale randomized controlled trials (RCTs) have been conducted for three diseases: age-related macular degeneration (AMD), cataracts, and dry eye.
The largest source of evidence is the Age-Related Eye Disease Study (AREDS) led by the U.S. National Eye Institute (NEI). AREDS, conducted from 1992 to 2001, was a large-scale RCT involving 3,640 participants 1), evaluating the “AREDS formulation” combining vitamin C 500 mg, vitamin E 400 IU, beta-carotene 15 mg, and zinc oxide 80 mg. It was shown to reduce the risk of AMD progression by approximately 25% in patients with moderate to advanced AMD (AREDS categories 3 and 4) 1).
In the AREDS2 study (4,203 cases) conducted from 2006 to 2012 2), the efficacy and safety of a new formulation replacing beta-carotene with 10 mg lutein + 2 mg zeaxanthin per day were verified. The replacement with lutein and zeaxanthin showed an effect equivalent to beta-carotene in suppressing AMD progression 2), while avoiding the increased risk of lung cancer in smokers associated with beta-carotene, making it the current standard formulation.
Importantly, the AREDS/AREDS2 formulation is intended to slow progression in patients with moderate to advanced AMD, and its efficacy in preventing the onset of AMD in the general population without AMD has not been established. Supplements are an adjunct to ophthalmic management, and the foundation is a combination of regular eye examinations for early detection and early treatment.
The AREDS formulation has established evidence of reducing the risk of progression of moderate to advanced AMD (AREDS categories 3 and 4) by approximately 25% 1). However, this is “progression suppression,” and the effect of “preventing onset” in healthy individuals without AMD has not been established at this time. There is no general recommendation for people without AMD risk, and consideration should be given to prescribing the AREDS2 formulation for patients confirmed to have moderate to advanced AMD.
The main supplement components related to eye diseases are broadly classified into five types.
Lutein and Zeaxanthin
Role: Main component of the pigment in the macula (the most important area at the center of the retina). It functions as a filter that absorbs blue light, scavenges reactive oxygen species (ROS), and protects the retina from photo-oxidative damage3).
Association with cataracts: Epidemiological studies have shown an inverse relationship between dietary intake of lutein and zeaxanthin and the risk of nuclear cataracts5).
Vitamin C and E
Role: Water-soluble (vitamin C) and fat-soluble (vitamin E) antioxidant vitamins. They reduce oxidative stress in the retinal pigment epithelium (RPE).
AREDS formulation dose: Vitamin C 500 mg + Vitamin E 400 IU/day1).
Cataract prevention: The Cochrane Review (Mathew 2012) concluded that the preventive effect of antioxidant supplements on cataracts is “not confirmed” 6). The AREDS study also found no significant preventive effect on cataracts.
Zinc
Role: Supports the metabolism of the retinal pigment epithelium as a cofactor for antioxidant enzymes (e.g., Cu/Zn-SOD, catalase)1).
Changes in AREDS2: A reduction to 25 mg was considered, but there was no significant difference from the 80 mg group2).
Omega-3 Fatty Acids (EPA/DHA)
AMD: In AREDS2, no additional effect of omega-3 fatty acids (DHA 350 mg + EPA 650 mg/day) on AMD was observed2). Epidemiological studies have reported an association between fish intake and reduced risk of AMD8).
Dry eye: In the DREAM study (535 patients, RCT), omega-3 supplements (EPA 2,000 mg + DHA 1,000 mg/day) showed no significant difference from olive oil placebo in improving dry eye symptoms7).
Anthocyanins found in blueberries and bilberries have been reported in basic research to improve dark adaptation and retinal blood flow. However, evidence of efficacy from RCTs is limited9), and at present, the evidence is considered insufficient to recommend in clinical practice.
The dosages of each formulation component are shown below.
Component
AREDS formulation
AREDS2 formulation
Vitamin C
500 mg/day
500 mg/day
Vitamin E
400 IU/day
400 IU/day
Beta-carotene
15 mg/day
Excluded (replaced with lutein/zeaxanthin)
Lutein
—
10 mg/day
Zeaxanthin
—
2 mg/day
Zinc oxide
80 mg/day
80 mg/day (25 mg also considered)
Copper oxide
2 mg/day
2 mg/day
QShould I take lutein supplements?
A
For patients diagnosed with moderate to advanced AMD (AREDS categories 3 and 4), the AREDS2 formulation (containing lutein 10 mg + zeaxanthin 2 mg per day) is recommended 2). On the other hand, there is no general recommendation for healthy individuals without AMD risk; dietary intake from green leafy vegetables such as spinach and kale is fundamental. It is important to make a decision after consulting an ophthalmologist.
Major change: replacement of beta-carotene with lutein 10 mg + zeaxanthin 2 mg/day
Results: Non-inferiority in suppressing AMD progression was demonstrated after substitution. In former smokers, the risk of progression to exudative AMD was further reduced in the lutein/zeaxanthin group.
Long-term follow-up of AREDS2 (2022, 10-year data)10):
In the lutein/zeaxanthin group, a further long-term reduction in the risk of progression to exudative AMD was confirmed.
The AREDS formulation was not confirmed to have a preventive effect against cataracts1). On the other hand, multiple epidemiological studies have shown an inverse association between dietary intake of lutein and zeaxanthin and the risk of nuclear cataracts5), suggesting that dietary intake may reduce the risk of cataract development. However, there are still no large-scale RCTs proving the interventional effect of supplements.
A Cochrane review (Mathew 2012, 21 RCTs) concluded that there is no reliable evidence that supplementation with antioxidant vitamins (A, C, E), lutein, and zeaxanthin delays the onset or progression of cataracts6).
The DREAM trial (2018) was an RCT comparing the efficacy of omega-3 fatty acids (EPA 2,000 mg + DHA 1,000 mg/day for 12 months) with an olive oil placebo in 535 patients with chronic dry eye. There was no significant difference between the two groups in the primary endpoint (OSDI [Ocular Surface Disease Index] score) 7), indicating a negative result for the efficacy of omega-3 supplements for dry eye. Although a meta-analysis (Giannaccare 2019) reported some efficacy 11), omega-3 supplements are not included in standard treatment for dry eye due to the high quality of the DREAM trial.
Indications: Patients diagnosed with moderate to advanced AMD (AREDS categories 3 and 4) in one eye2)
Limited effect on early AMD: AREDS categories 1 and 2 (small drusen) have not shown significant progression suppression. Unnecessary supplement use poses a risk of excessive intake, so caution is needed.
Confirmation of smoking status: For smokers, choose the AREDS2 formulation without beta-carotene.
Nillerdk. Spinach leaves (1 kg, separated from stems). Wikimedia Commons. 2008. Figure 1. Source ID: commons.wikimedia.org/wiki/File:Spinach_leaves.jpg. License: CC BY 3.0.
Spinach leaves, excluding stems, are a representative source of lutein and zeaxanthin, containing about 12 mg/100 g of lutein. This corresponds to dietary intake from green-yellow vegetables (spinach, kale) rich in lutein, as discussed in the section “4. Actual Intake” of the text.
Green and yellow vegetables are excellent sources of lutein and zeaxanthin4).
Spinach: lutein about 12 mg/100 g, zeaxanthin about 1.1 mg/100 g4)
Kale: Approximately 22 mg/100 g of lutein (highest level among foods) 4)
Broccoli: about 1.4 mg of lutein per 100 g4)
Egg yolk: High bioavailability of lutein and zeaxanthin (3–4 times that of vegetables) 4)
Consuming fish (such as mackerel, Pacific saury, and sardines) at least twice a week is useful as a source of EPA/DHA8), and epidemiological studies have reported an association between fish intake and reduced risk of AMD.
Supplements are classified as food, not medicine. Under the Consumer Affairs Agency’s system for Foods with Function Claims (established in 2015), they are allowed to display functional claims based on certain scientific evidence12), but they have not undergone national review for efficacy and safety like pharmaceuticals. When selecting products equivalent to the AREDS2 formulation, check the ingredient content and be careful not to exceed the recommended intake.
QWhat foods contain high levels of lutein?
A
Green leafy vegetables such as spinach (about 12 mg/100 g), kale (about 22 mg/100 g), and broccoli are major dietary sources of lutein 4). Egg yolks, while not as high in lutein content as vegetables, have high absorption efficiency due to their fat solubility. A daily intake of 6–10 mg of lutein from food is recommended. Actively consuming green leafy vegetables every day is the basis for obtaining lutein from the diet.
If supplements are not used properly, they can cause side effects and risks. The following points require attention.
Beta-carotene and lung cancer risk in smokers:
In the ATBC study (1994), beta-carotene supplementation (20 mg/day) in 29,133 male smokers increased lung cancer incidence by 18% 13)
In the CARET study, beta-carotene supplementation increased the risk of lung cancer in smokers and asbestos-exposed individuals.
In AREDS2, based on this finding, beta-carotene was replaced with lutein/zeaxanthin 2)
Do not use AREDS formulations containing beta-carotene in smokers or individuals with a history of smoking, even after quitting.
Excessive zinc intake:
Copper deficiency anemia has been reported with long-term use of 80 mg/day of zinc oxide in the AREDS formulation1)
The AREDS formulation contains 2 mg of copper oxide to prevent copper deficiency, but regular blood tests are recommended during long-term use.
Tolerable upper intake level of zinc for general adults (Japanese Dietary Intake Standards 2020 edition): 45 mg/day for men, 35 mg/day for women
High-dose vitamin E intake:
Schürk et al. (2010, meta-analysis) suggested an association between high-dose vitamin E intake and increased risk of hemorrhagic stroke14)
Long-term use of high doses (400 IU/day) requires caution
Drug interactions:
Vitamin E and omega-3 fatty acids have anticoagulant effects, so caution is needed regarding interactions with anticoagulants such as warfarin.
Consult your doctor about discontinuing use before surgery.
QDo eye supplements have side effects?
A
Beta-carotene in the AREDS formulation increases the risk of lung cancer in smokers, so it is contraindicated for current or former smokers 13). The AREDS2 formulation avoids this risk by replacing beta-carotene with lutein/zeaxanthin. Additionally, long-term use of 80 mg/day zinc oxide can cause copper deficiency anemia, so the formulation always includes 2 mg copper oxide 1). High-dose long-term vitamin E intake has been associated with an increased risk of hemorrhagic stroke 14), requiring caution.
The macula is an area at high risk for light-induced oxidative stress, and ultraviolet and blue light can generate reactive oxygen species (ROS). Oxidative stress is involved in the onset and progression of AMD3).
ROS production: Photooxidation of lipofuscin (waste product) due to light reactions is the main cause of RPE damage
Drusen formation: Lipoproteins and complement deposit in the extracellular matrix due to decreased processing capacity of the RPE
Progression to wet AMD: Oxidative stress and RPE damage induce complement activation and VEGF signaling, leading to neovascularization
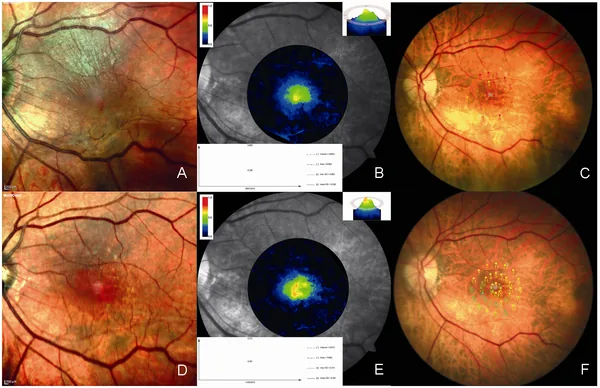
Romano MR, Cennamo G, Grassi P, et al. Changes in macular pigment optical density after membrane peeling. PLoS One. 2018;13(5):e0197034. Figure 1. PMID: 29758035; PMCID: PMC5951543; DOI: 10.1371/journal.pone.0197034. License: CC BY 4.0.
A pseudo-color map visualizing macular pigment optical density (MPOD), showing high density (warm colors) of pigment distribution in the fovea. This corresponds to the photoprotective and antioxidant functions of MPOD formed by lutein and zeaxanthin, discussed in Section 6: Pathophysiology and Antioxidant Mechanisms.
Lutein and zeaxanthin selectively accumulate in the macula, forming the macular pigment optical density (MPOD)3).
Optical filter function: Selectively absorbs blue light (400–500 nm) and reduces its arrival at photoreceptors
Antioxidant function: Functions as a ROS scavenger that directly eliminates singlet oxygen and peroxy radicals
Meso-zeaxanthin: The third macular pigment enzymatically converted from lutein within the retina, with the highest concentration in the central macula3)
Role of Zinc as a Cofactor for Antioxidant Enzymes
Zinc functions as an essential cofactor in the active site of the antioxidant enzyme Cu/Zn-SOD (copper-zinc superoxide dismutase)1). SOD converts superoxide anions, a type of ROS, into harmless hydrogen peroxide. It also works together with catalase and glutathione peroxidase to maintain the overall antioxidant defense system. The RPE is a highly metabolic tissue that processes phagosomes shed from photoreceptors, and an adequate supply of zinc is important for maintaining normal function.
DHA (docosahexaenoic acid) is an omega-3 long-chain polyunsaturated fatty acid abundantly present in the outer segment membranes of retinal photoreceptors. Along with EPA (eicosapentaenoic acid), it serves as a precursor for the anti-inflammatory lipid mediators resolvins and protectins 7). These mediators promote the resolution of inflammation, but clinical effects on dry eye in RCTs are considered insufficient.
Long-term follow-up data from AREDS2 over 10 years (Report 28: Chew 2022) 10) confirmed that the lutein/zeaxanthin group further reduced the risk of progression to exudative AMD in the long term. No long-term safety issues were observed, and the benefit of a beta-carotene-free formulation for smokers was reaffirmed.
Utilization of Macular Pigment Optical Density (MPOD) as a Biomarker
MPOD measurement is being studied as an indicator of macular carotenoid levels 3). Evaluation using heterochromatic flicker photometry, resonance Raman spectroscopy, and fundus autofluorescence is being investigated as an objective measure of supplement efficacy.
Personalized nutritional guidance based on genetic polymorphisms
Research suggests that the effectiveness of the AREDS formulation may vary depending on polymorphisms in AMD susceptibility genes (CFH Y402H and ARMS2 A69S)15). It has been indicated that individuals carrying CFH polymorphisms may have different responses to zinc15), and in the future, personalized supplement prescriptions based on genetic profiles may become possible.
Basic research has accumulated showing that the composition of the gut microbiota affects the absorption efficiency and blood concentration of lutein and zeaxanthin. It is known that even with the same diet and supplement intake, there are large individual differences in blood lutein levels, and strategies to improve absorption efficiency through combination with gut environment improvement (e.g., probiotics) are being explored.
Ongoing Research on Nutritional Interventions for Dry Eye
Although the DREAM study negated the effect of omega-37), research is progressing on the association between overall dietary patterns (such as the Mediterranean diet) and dry eye risk11). The involvement of other nutrients such as polyphenols and vitamin D in dry eye is also being investigated, and new RCTs are being conducted.
Age-Related Eye Disease Study Research Group.. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417-1436. doi:10.1001/archopht.119.10.1417. PMID:11594942; PMCID:PMC1462955.
Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013;309(19):2005-15. doi:10.1001/jama.2013.4997. PMID:23644932.
Bernstein PS, Li B, Vachali PP, Gorusupudi A, Shyam R, Henriksen BS, et al. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Progress in retinal and eye research. 2016;50:34-66. doi:10.1016/j.preteyeres.2015.10.003. PMID:26541886; PMCID:PMC4698241.
Perry A, Rasmussen H, Johnson EJ. Xanthophyll (lutein, zeaxanthin) content in fruits, vegetables and corn and egg products. J Food Compos Anal. 2009;22(1):9-15. doi:10.1016/j.jfca.2008.07.006.
Christen WG, Liu S, Glynn RJ, Gaziano JM, Buring JE.. Dietary carotenoids, vitamins C and E, and risk of cataract in women: a prospective study. Arch Ophthalmol. 2008;126(1):102-109. doi:10.1001/archopht.126.1.102. PMID:18195226; PMCID:PMC2396535.
Mathew MC, Ervin AM, Tao J, Davis RM. Antioxidant vitamin supplementation for preventing and slowing the progression of age-related cataract. The Cochrane database of systematic reviews. 2012;2012(6):CD004567. doi:10.1002/14651858.CD004567.pub2. PMID:22696344; PMCID:PMC4410744.
Dry Eye Assessment and Management Study Research Group, Asbell PA, Maguire MG, Pistilli M, Ying GS, Szczotka-Flynn LB, Hardten DR, Lin MC, Shtein RM.. n-3 Fatty Acid Supplementation for the Treatment of Dry Eye Disease. N Engl J Med. 2018;378(18):1681-1690. doi:10.1056/nejmoa1709691. PMID:29652551; PMCID:PMC5952353.
SanGiovanni JP, Chew EY, Clemons TE, Davis MD, Ferris FL, Gensler GR, Kurinij N, Lindblad AS, Milton RC, Seddon JM, Sperduto RD, Age-Related Eye Disease Study Research Group.. The relationship of dietary lipid intake and age-related macular degeneration in a case-control study: AREDS Report No. 20. Arch Ophthalmol. 2007;125(5):671-679. doi:10.1001/archopht.125.5.671. PMID:17502507.
Kalt W, Hanneken A, Milbury P, Tremblay F. Recent research on polyphenolics in vision and eye health. Journal of agricultural and food chemistry. 2010;58(7):4001-7. doi:10.1021/jf903038r. PMID:20102149.
Chew EY, Clemons TE, Agrón E, Domalpally A, Keenan TDL, Vitale S, Weber C, Smith DC, Christen W, AREDS2 Research Group.. Long-term Outcomes of Adding Lutein/Zeaxanthin and ω-3 Fatty Acids to the AREDS Supplements on Age-Related Macular Degeneration Progression: AREDS2 Report 28. JAMA Ophthalmol. 2022;140(7):692-698. doi:10.1001/jamaophthalmol.2022.1640. PMID:35653117; PMCID:PMC9164119.
Giannaccare G, Pellegrini M, Sebastiani S, Bernabei F, Roda M, Taroni L, et al. Efficacy of Omega-3 Fatty Acid Supplementation for Treatment of Dry Eye Disease: A Meta-Analysis of Randomized Clinical Trials. Cornea. 2019;38(5):565-573. doi:10.1097/ICO.0000000000001884. PMID:30702470.
消費者庁. 機能性表示食品制度の概要. 2015.
Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med. 1994;330(15):1029-1035. doi:10.1056/nejm199404143301501.
Schürks M, Glynn RJ, Rist PM, Tzourio C, Kurth T. Effects of vitamin E on stroke subtypes: meta-analysis of randomised controlled trials. BMJ (Clinical research ed.). 2010;341:c5702. doi:10.1136/bmj.c5702. PMID:21051774; PMCID:PMC2974412.
Seddon JM, Reynolds R, Yu Y, Daly MJ, Rosner B. Risk models for progression to advanced age-related macular degeneration using demographic, environmental, genetic, and ocular factors. Ophthalmology. 2011;118(11):2203-11. doi:10.1016/j.ophtha.2011.04.029. PMID:21959373; PMCID:PMC4097877.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.