Corneal nerve thickening (prominent corneal nerves) refers to a condition in which the corneal nerves within the stroma, normally visible only in the peripheral cornea by slit-lamp microscopy, appear thick and prominent extending to the central cornea or pupillary area.
The cornea is one of the most densely innervated tissues in the human body, with a density of free nerve endings 300 to 600 times that of the skin 2). The sensory nerves of the cornea originate from the first branch of the trigeminal nerve (ophthalmic nerve V1). The long posterior ciliary nerves, branches of the nasociliary nerve, penetrate the sclera and enter the stroma at the limbus. After running radially within the stroma, they penetrate Bowman’s layer and supply free nerve endings to all layers of the epithelium.
In healthy individuals, the thickest corneal stromal nerves (axon bundles) are observed by slit-lamp microscopy only in the peripheral one-third of the cornea. If thickened nerves are found in the central cornea, it may be an early sign of an important systemic disease. In particular, detecting undiagnosed MEN2B can lead to life-saving prophylactic total thyroidectomy, making the search for the cause of corneal nerve thickening extremely important.
QIs corneal nerve thickening always a pathological finding?
A
Observation of thick nerve trunks in the extreme periphery of the cornea is normal and not pathological. Clinically significant “corneal nerve thickening” refers to cases where thick nerves extend into the central cornea or pupillary area, where they are not normally visible. However, mild thickening may be a normal variant and should be evaluated together with other clinical findings and systemic symptoms.
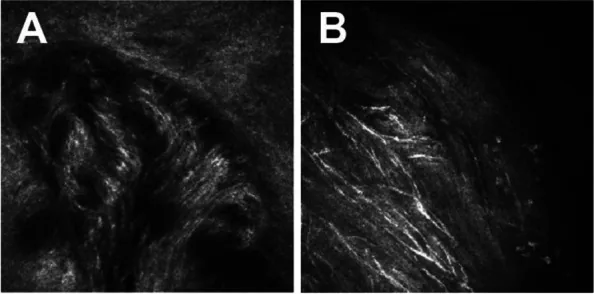
BMC Ophthalmol. 2023 Jun 12; 23:260. Figure 4. PMCID: PMC10258932. License: CC BY.
Microscopic image showing thick and clearly visible corneal nerves. Thickening and tortuosity of nerve fibers running through the stroma are emphasized.
Slit-lamp microscopy findings: Observed as thick white linear structures running within the corneal stroma. They usually extend radially from the limbus toward the center, with branching. In MEN2B, they often reach the pupillary area.
IVCM findings: Allows evaluation of corneal nerve microstructure at up to 800x magnification. In MNS cases, a hyperreflective thickened nerve plexus is seen in the anterior stroma, showing branching, loop formation, and nodular dilation 1)
Associated findings (MEN2B): Wavy thickening and ectropion of the eyelid margin due to mucosal neuromas, conjunctival neuromas, dry eye (in 67% of carriers)
In addition, corneal nerve thickening has also been reported in Riley-Day syndrome (familial dysautonomia), lipid proteinosis (hyalinosis cutis et mucosae), and congenital ichthyosis.
QHow to differentiate MEN2B from MNS (mucosal neuroma syndrome)?
A
Both are clinically similar in that they present with thickened corneal nerves and mucosal neuromas, but MNS lacks RET gene mutations and is not associated with endocrine tumors such as medullary thyroid carcinoma or pheochromocytoma. In MNS, a frameshift mutation in the SOS1 gene has been reported 1). RET genetic testing is essential for differentiation and is extremely important in determining the need for prophylactic total thyroidectomy.
Slit-lamp microscopy: Systematically observe the entire cornea to evaluate the presence of thickened nerves reaching the central area. Magnification is up to about 40x, and only thick stromal nerves can be observed.
In vivo confocal microscopy (IVCM): Non-invasively evaluates the microstructure of corneal nerves at up to 800x magnification. Nerve density, course pattern, branching, loop formation, and nodular dilation can be quantified 1).
RET genetic testing: Performed when MEN2 is suspected. Essential for definitive diagnosis of MEN2B.
Endocrine screening: Includes calcitonin measurement, thyroid ultrasound, and adrenal MRI.
Systemic examination: Check for oral mucosal neuromas, Marfanoid habitus, café-au-lait spots, Lisch nodules, and skin findings.
There are findings that resemble thickening of the corneal nerves.
Similar findings
Key points for differentiation
Ghost vessels
Vascular origin; thicker and whiter
Lattice lines (lattice dystrophy)
More opaque and overlapping
Waite-Beckham lines
Deep vertical lines at the level of Descemet’s membrane
Radial keratoneuritis is typical of Acanthamoeba keratitis, but has also been reported in Pseudomonas aeruginosa keratitis, so it is not entirely pathognomonic.
MEN2B/2A: Prophylactic total thyroidectomy is the most important intervention. If detected before metastasis of medullary thyroid carcinoma, surgery can be curative. There are many case reports of early detection of medullary thyroid carcinoma after ophthalmologists referred patients based on corneal nerve thickening.
MNS: Since there is no RET mutation and the risk of endocrine tumors is low, prophylactic total thyroidectomy is not mandatory 1). Regular follow-up and genetic counseling are recommended.
Refsum disease: Progression of symptoms is suppressed by restricting phytanic acid in the diet.
Acanthamoeba keratitis: Requires long-term topical therapy with polyhexamethylene biguanide (PHMB) or chlorhexidine. Surgical intervention is sometimes necessary.
Keratoconus: Treatment is performed according to the stage of progression, including contact lenses, corneal cross-linking, and corneal transplantation3).
QWhy is early detection of MEN2B important?
A
In MEN2B, almost 100% of mutation carriers develop medullary thyroid carcinoma, which can be fatal if untreated. Corneal nerve thickening can be observed as early as age 2, so ophthalmological findings often provide the first clue for diagnosing MEN2B. Prophylactic total thyroidectomy before metastasis can achieve a cure, and detection of corneal nerve thickening can literally save the patient’s life.
The sensory nerves of the cornea originate from the first branch of the trigeminal nerve (ophthalmic nerve V1). Nerves entering the stroma from the limbus run through the anterior two-thirds of the stroma, then penetrate Bowman’s layer and form the sub-basal nerve plexus just below the epithelial basal cell layer2).
Approximately 60% of corneal sensory nerves contain calcitonin gene-related peptide (CGRP), and about 20% contain substance P2). Electrophysiologically, they are classified into three types.
Mechanoreceptors/mechanical nociceptors (about 20%): Respond to mechanical stimuli.
Polymodal nociceptors (about 70%): Respond to mechanical, chemical, and thermal stimuli, and are the main driving force for reflex tear secretion2).
Cold receptors (approximately 10–15%): respond to temperature changes
The morphological basis of thickened corneal nerves varies depending on the underlying disease.
MEN2B: Mutations in the RET proto-oncogene cause proliferation of axons and Schwann cells in neural crest-derived tissues. The number of corneal nerve axons and Schwann cells increases, leading to an increase in nerve bundle diameter.
MNS: A frameshift mutation in the SOS1 gene is involved 1). Although RET mutations are not present, the phenotype includes corneal nerve thickening similar to MEN2B.
Acanthamoeba keratitis: The protozoan spreads along corneal nerves, causing perineural inflammatory infiltration. This is observed as radial keratoneuritis.
Abnormal myelination: When nerve fibers that are normally unmyelinated within the cornea become abnormally myelinated, light reflection increases, giving a thickened appearance.
Yin et al. reported the case of a 41-year-old man with thickened corneal nerves and conjunctival neuromas but no RET mutation 1).
Genetic testing identified a heterozygous frameshift mutation (c.3263dup) in the SOS1 gene. Endocrine screening revealed a mild elevation of calcitonin, but thyroid imaging and head CT/MRI detected no obvious neoplastic lesions 1).
This report indicates that when corneal nerve thickening and mucosal neuromas are present, not only MEN2B but also the possibility of MNS should be considered 1). Since prophylactic total thyroidectomy is not mandatory in MNS, accurate differentiation is important to avoid excessive invasive interventions.
In vivo confocal microscopy (IVCM) is becoming established as a non-invasive, high-resolution technique for evaluating corneal nerve morphology 1). In the future, quantitative indicators such as corneal nerve density, diameter, and branching patterns may be used for screening and monitoring systemic diseases.
Yin L, Wang Y, Zhu J, Tan CY, Sun C, Yao Y. Prominent corneal nerves in pure mucosal neuroma syndrome, a clinical phenotype distinct from multiple endocrine neoplasia type 2B. BMC ophthalmology. 2023;23(1):260. doi:10.1186/s12886-023-03005-0. PMID:37303040; PMCID:PMC10258932.
Dartt DA. Neural regulation of lacrimal gland secretory processes: relevance in dry eye diseases. Progress in retinal and eye research. 2009;28(3):155-77. doi:10.1016/j.preteyeres.2009.04.003. PMID:19376264; PMCID:PMC3652637.
Jhanji V, Ahmad S, Amescua G, et al. Corneal Ectasia Preferred Practice Pattern. Ophthalmology. 2024 Apr;131(4):P205-P246. doi:10.1016/j.ophtha.2023.12.038. PMID:38349299.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.