Linear interstitial keratitis (LIK) is a rare corneal disease that causes linear opacities in the corneal stroma. It has been reported in young adults as early as 1923.
Previously, it was thought to be caused by syphilis infection. However, accumulated case reports have shown that anti-treponemal antibodies are generally negative. Positive serological tests are considered incidental findings. Histological examination of patch grafts in cases of corneal perforation has not yielded definitive findings.
Syphilitic interstitial keratitis has long been known as one of Hutchinson’s triad (Hutchinson teeth, interstitial keratitis, deafness) in congenital syphilis 1). However, LIK is positioned as an independent disease entity clinically distinct from syphilitic interstitial keratitis.
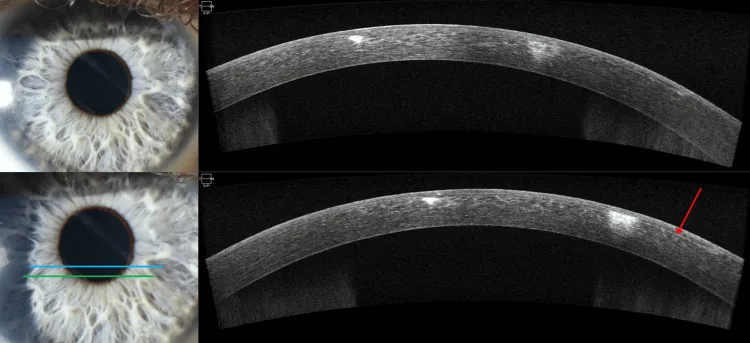
Luis C Barrientos, Michael Wildes Linear Interstitial Keratitis: A Report of Two Cases and Review of Literature 2025 Mar 22 Cureus.; 17(3):e80985 Figure 4. PMCID: PMC12010693. License: CC BY.
In the anterior segment photograph on the left, the blue and green lines indicate the OCT scan positions. The OCT on the right shows a linear hyperreflective band within the corneal stroma, with the lesion running along the sub-flap stroma.
Main complaints are blurred vision, tearing, pain, and redness. Symptoms often occur unilaterally. The condition is characterized by recurrent episodes of remission and relapse.
Historically, associations with syphilis and Lyme disease have been suspected. However, serological test results are inconsistent and not all cases show clear positivity. Autoimmune involvement has been proposed but has not yet been proven.
Syphilitic interstitial keratitis typically presents as bilateral non-ulcerative corneal opacities in late childhood to young adulthood 1). Unlike LIK, it is characterized by tearing and photophobia, poor response to systemic penicillin, and responsiveness to steroids 1).
QIs there a relationship between syphilis and LIK?
A
Historically, syphilis was suspected as a cause of LIK, but this is now considered unlikely. Serological tests in LIK patients generally do not show anti-treponemal antibodies. Syphilitic interstitial keratitis is a different disease presenting with bilateral non-ulcerative corneal opacities and has a different clinical picture from LIK.
The diagnosis of LIK is based on clinical findings. The linear appearance of corneal opacity is the most important diagnostic clue.
Key diagnostic points:
Confirm linear opacities within the corneal stroma using a slit-lamp microscope.
Responsiveness to steroid eye drops supports the diagnosis.
If epithelial defects are present, culture tests should be performed, but usually no bacterial growth is observed.
Differential diagnoses:
Differential Diagnosis
Key Differentiating Features
Herpetic disciform keratitis
Round stromal edema, greasy keratic precipitates
Necrotizing keratitis
Severe inflammation, necrotic findings
Infectious keratitis
Infiltrates, positive culture
In the differential diagnosis of corneal stromal opacity, it is important to distinguish and evaluate four elements: edema, infiltration, deposition, and scarring. In LIK, inflammatory edema and infiltration are predominant.
QHow is it differentiated from other types of keratitis?
A
The most characteristic feature of LIK is that the corneal opacity shows a “linear” pattern. In herpetic keratitis, disciform edema is typical, and in infectious keratitis, infiltrative foci or positive culture findings are seen. LIK responds well to steroid eye drops, which is also useful for differentiation. However, it is important to rule out infectious keratitis, and culture tests should be performed as needed.
Steroid eye drops (e.g., betamethasone, fluorometholone) are the first-line treatment.
The potency and frequency of steroid eye drops are adjusted according to the degree of inflammation.
After symptom improvement, the dose is gradually reduced, aiming for discontinuation while monitoring for recurrence.
Surgical Treatment:
Full-thickness corneal transplantation is considered only when corneal perforation occurs.
In the usual course, surgery is not indicated.
Prognosis: Recovery with steroid use is generally favorable. However, inflammation tends to recur, and the course may involve repeated relapses and remissions. Long-term prognosis varies by case.
QWill it recur if I stop steroids?
A
LIK tends to recur and remit. Abrupt discontinuation of steroid eye drops can trigger recurrence, so it is important to gradually reduce the dose as directed by your doctor. Even if it recurs, restarting steroid eye drops can be expected to improve the condition.
The corneal stroma is composed of regularly arranged collagen fibers, and this regularity maintains corneal transparency. In LIK, inflammation occurs in the stroma in a linear pattern, increasing the water content between collagen fibers and leading to loss of transparency.
Proposed mechanisms:
Autoimmune theory: Petrovic et al. have proposed autoimmune involvement. An immune response to antigens in the corneal stroma may occur in a linear pattern, but this has not been proven.
Infection-related theory: Syphilis and Lyme disease were previously suspected, but serological tests have ruled them out.
Comparison with syphilitic interstitial keratitis is useful for understanding the pathology. Syphilitic interstitial keratitis occurs as a late symptom of congenital syphilis and is one of Hutchinson’s triad 1). The corneal lesions are resistant to systemic penicillin but respond to steroids 1). This feature is shared with LIK’s steroid responsiveness, but LIK essentially lacks positive serological findings for syphilis.
Reports on LIK are limited, but recent advances in imaging diagnostics are deepening our understanding of the pathology.
Evaluation by confocal microscopy: Detailed histological observation of LIK using in vivo confocal microscopy has been reported. It allows non-invasive assessment of inflammatory cell infiltration and structural changes in the corneal stroma.
Chauhan K, Fonollosa A, Giralt L, Artaraz J, Randerson EL, Goldstein DA, et al. Demystifying Ocular Syphilis - A Major Review. Ocul Immunol Inflamm. 2023;31(7):1425-1439. doi:10.1080/09273948.2023.2217246. PMID:37307579.
Barrientos LC, Wildes M. Linear Interstitial Keratitis: A Report of Two Cases and Review of Literature. Cureus. 2025;17(3):e80985. PMID: 40260341.
Calvo CM, Sikder S, Mamalis N, Mifflin MD. Linear interstitial keratitis: a distinct clinical entity revisited. Cornea. 2012;31(12):1500-3. PMID: 22406946.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.