Solar retinopathy (SR) is a photic maculopathy caused by sunlight. It can occur not only in people with mental illness or in those who stare at the sun for religious reasons, but also from improper use of equipment when observing a solar eclipse. Concentration of intense light energy on the fovea causes phototoxic retinal damage, and it is also called eclipse retinopathy.1)
The causes are varied.1)
Naked-eye observation of a solar eclipse: observing a solar eclipse using improper filters such as a desk underlay is the classic cause
Looking directly at the sun: includes intentional staring by people with mental illness or for religious reasons
Welding work: exposure to ultraviolet light without proper protection
Laser pointers: injury from green or blue lasers
Sunlight therapy / sunbathing: prolonged exposure to strong sunlight
Reflected light from mobile devices: accidental retinal injury through a smartphone camera lens5)
Spontaneous recovery often occurs within 3 to 6 months after onset, but some cases leave permanent vision loss.1) Younger people are more likely to be affected than older people because the lens transmits more light and the pupil is larger.
QCan even a brief look at the eclipse cause retinopathy?
A
Even for a few seconds without a protective filter, focused ultraviolet and visible light can reach the fovea and cause phototoxic injury. On a clear day, even about 1 second of staring can cause damage. It is essential to use eclipse glasses certified to ISO 12312-2.2)
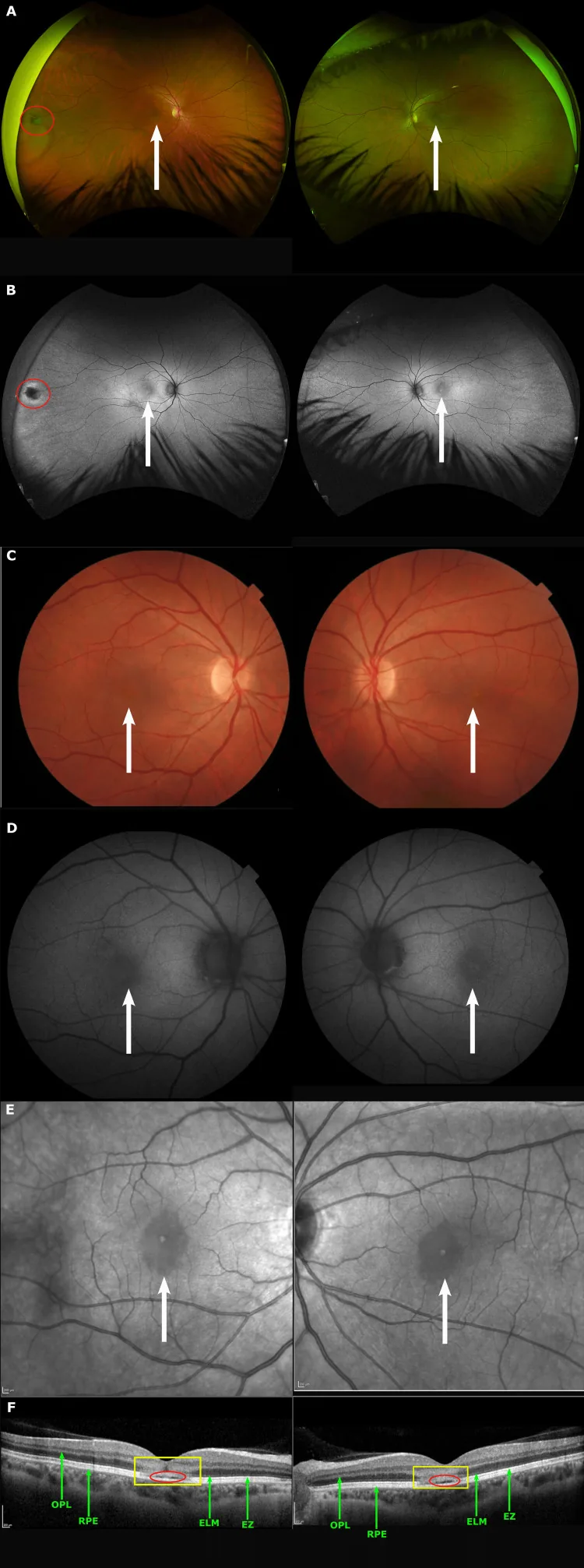
(A)(C) Fundus photographs, (B)(D) autofluorescence, and (E) a near-infrared image show a foveal lesion (white arrows). In (F), OCT shows a hyperreflective area extending from the outer plexiform layer to the retinal pigment epithelium layer (yellow box) and attenuation of each layer (red circles). This corresponds to the foveal lesion discussed in section 2, Main symptoms and clinical findings.
Symptoms appear within several hours to a few days after exposure to light.1)2) In photochemical injury, there may be no abnormality immediately after the injury, and symptoms may appear days later.
Decreased central vision: The most common symptom. It ranges from mild to severe
Central scotoma: A black or gray missing area is felt in the center
Metamorphopsia (distorted vision): Caused by disorganization of the foveal photoreceptors
Color vision abnormality: Blue-green color perception is especially likely to be affected
Feeling unwell: This may occur as a general symptom in the acute phase.
In cases with strong sunlight exposure at high altitude, several people developed symptoms at the same time, and the increased amount of ultraviolet light was involved in the cause.4)
OCT is the most important test for diagnosing and following solar retinopathy.1)2) In the early stage after injury, a yellow spot about 160 μm in diameter may be seen at the fovea, and it often disappears within 1 to 2 weeks. OCT findings change depending on the stage of the disease.
Acute phase
Disruption or loss of the ellipsoid zone (IS/OS junction): Seen directly beneath the fovea. This is the most characteristic finding.
Hyperreflective lesion: A small lesion seen in the outer nuclear layer to photoreceptor layer.
Thinning of the outer retinal layers: Reflects structural changes around the fovea.
Recovery phase
Partial regeneration of the ellipsoid zone: The disrupted area shrinks over several weeks to several months.
Reduction and disappearance of hyperreflective lesions: Reflects the repair process in the outer layers.
Persistent subtle changes: In cases where the changes do not disappear completely, vision impairment continues.
Chronic phase
Foveal cyst-like change / pseudocyst: A lasting change seen in some cases.
Destruction of the Verhoeff membrane (IZ layer): Specific to certain phototoxic patterns.1)
Full-thickness defect (full-size defect): The final appearance in severe cases. Poor visual prognosis.
Microperimetry can quantitatively assess foveal function.
In a photographer’s bilateral solar retinopathy case, the size of the central scotoma and the drop in residual sensitivity were recorded.2)
QCan symptoms occur in only one eye?
A
Depending on how directly the light hits and whether protective eyewear was used, it can be unilateral or bilateral. Bilateral onset has been reported in photographers exposed to sunlight.2)
For each cause of solar retinopathy, the light’s wavelength, intensity, and exposure circumstances differ.1)
Solar eclipse viewing: Unprotected naked-eye viewing of a partial solar eclipse is the most common. It can also occur during a total eclipse from exposure during the transition phase
Welding arc: Mainly ultraviolet light. It can occur without a protective mask or even from a brief glance
Laser pointers: coherent green (532 nm) and blue (445 nm) light are especially dangerous1)
Sunlight at high altitude: the thinner atmosphere increases ultraviolet exposure4)
“Staring at the sun” challenge on social media: a dangerous act that can draw in young people2)
Reflected light from mobile devices: indirect concentration of sunlight through a smartphone lens5)
In diagnosis, asking about a history of solar viewing is the most important one. Weather is an important factor; even a one-second stare on a clear day can cause damage. Check the following items.
History of solar viewing (eclipse, looking directly at the sun, religious practices, occupational exposure)
Weather, time of day, and whether a filter was used at the time of observation
Time from injury to symptom onset (photochemical injury may be delayed by several days)
OCT is the most important test in diagnosing solar retinopathy. 1)
It can evaluate changes in the outer layers (ellipsoid zone, outer nuclear layer, photoreceptor layer) at high resolution.
It is useful for staging, predicting visual prognosis, and follow-up.
Fundus autofluorescence (FAF): Visualizes changes in the metabolic activity of the RPE (retinal pigment epithelium). It may show hyperfluorescence in the acute phase and hypofluorescence in the chronic phase
There is no effective treatment for solar retinopathy. Many cases recover on their own.
In a photographer with bilateral solar retinopathy, visual acuity improved 3 months after taking photos without an appropriate protective filter. 2) The spontaneous recovery rate has been reported to be 50–83%. 2)
The main treatment options and their evaluations are shown below.
Treatment
Assessment
Notes
Observation
First-line
Most recover spontaneously in 3–6 months
Systemic steroid therapy
Uncertain; risk present
Effect is unclear. Risk of inducing CSCR2)3)
Antioxidants (such as vitamins C and E)
Theoretical rationale only
In vitro studies have reported inhibition of damage, but the effect of taking it after injury is unclear1)
If a permanent central scotoma remains, using low-vision aids and training in eccentric fixation may be helpful.
QWill vision recover without treatment?
A
In many cases, vision improves over 3 to 6 months on its own. Recovery rates of 50 to 83% have been reported, but severe phototoxicity or delayed medical attention can leave lasting vision loss.2)
6. Pathophysiology and detailed mechanism of onset
Blue light is absorbed by lipofuscin in retinal pigment epithelial cells and by visual pigments in photoreceptors
A2E (N-retinylidene-N-retinylethanolamine), a lipofuscin component, acts as a photosensitizer
Large amounts of reactive oxygen species (ROS), such as singlet oxygen, are generated
Normally, reactive oxygen species are cleared by enzymes and antioxidants, but with excessive light exposure, lipid peroxidation of the photoreceptor membrane progresses and damages photoreceptors and retinal pigment epithelial cells
Oxidative damage occurs in the outer segment and cell membranes of photoreceptors2)
With photochemical injury, the fundus is normal immediately after injury, and symptoms and macular degeneration appear a few days later.
If the light is intense enough, such as when looking directly at the midsummer southern sky for a short time, heat conversion in the retina causes immediate coagulative damage. In thermal injury, symptoms and a coagulation spot in the macula are seen immediately after injury.
In mild to moderate injury, if the photoreceptor nuclei (outer nuclear layer) are preserved, the outer segments can regenerate.5)
In the mobile-device reflected-light cases reported by Marticorena et al. (2022), partial recovery of the outer segments was observed after phototoxic injury with preservation of the photoreceptor nuclei.5)
When injury is severe and progresses to cystic change or full-thickness loss, tissue regeneration is limited and can lead to permanent visual impairment. Damage ranges from no fundus abnormalities to residual chorioretinal atrophy.
Multimodal assessment combining OCT, fundus autofluorescence, mfERG, and microperimetry is being studied as a biomarker for disease staging and visual prognosis prediction.1)2)
In particular, the relationship between the extent of ellipsoid zone damage and remaining visual acuity is being examined.1)
Retinal injury from sunlight focused through a smartphone camera lens was reported for the first time in the world in 2022.5)
As mobile devices become more widespread, the risk of accidental exposure is increasing, especially in young people and during outdoor activities.
The need for preventive education tailored to this new form of exposure has been proposed.5)
Based on the mechanism of ROS-mediated photochemical damage, the therapeutic potential of antioxidants (vitamin C, vitamin E, lutein) and neuroprotective drugs is being considered in theory. In vitro, antioxidants such as vitamin C have been reported to reduce damage, but the effect of taking them after injury is unclear, and evidence showing clinical effectiveness is currently insufficient.1)
QCould a treatment for solar retinopathy be established in the future?
A
Research on antioxidant therapy and neuroprotective therapy for photochemical damage is progressing, and early intervention after onset is thought to be important. At present, there is no established treatment, and prevention is the most important measure.1)
Timofte Zorila MM, Vitiello L, Lixi F, et al. Photic Retinopathy: Diagnosis and Management of This Phototoxic Maculopathy. Life (Basel). 2025;15(4):639. doi:10.3390/life15040639.
Gabriel A, Dimitry RS, Milad M, Kelada M, Papastavrou K. A Case of Bilateral Macular Phototoxicity and the Role of Multimodal Imaging. Cureus. 2025;17(12):e99791. doi:10.7759/cureus.99791.
Sharma R, et al. Solar retinopathy at high altitude: report of three cases with increased ultraviolet exposure. High Alt Med Biol. 2021.
Marticorena J, Honrubia A, Ascaso J. Solar maculopathy secondary to sunlight exposure reflected from the screen of mobile devices: two case reports. J Med Case Rep. 2022;16(1):360. doi:10.1186/s13256-022-03567-5.
Copy the article text and paste it into your preferred AI assistant.
Article copied to clipboard
Open an AI assistant below and paste the copied text into the chat box.